

Feasibility of a Biomarker-Based Screening for Pre-Symptomatic AL Amyloidosis in Patients With Intermediate/High-Risk MGUS
- PMID: 39627959
- PMCID: PMC11705207
- DOI: 10.1002/ajh.27545
Feasibility of a Biomarker-Based Screening for Pre-Symptomatic AL Amyloidosis in Patients With Intermediate/High-Risk MGUS
Abstract
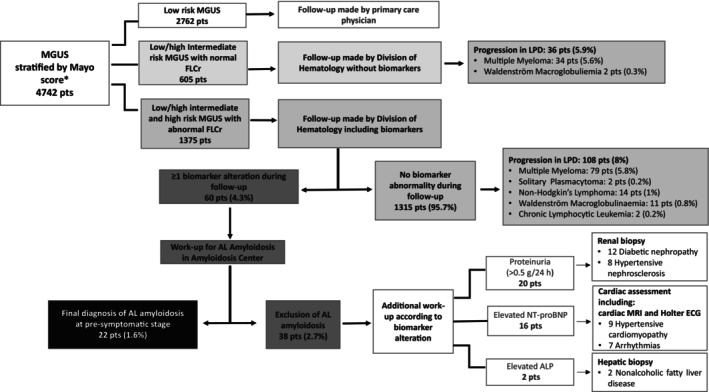
Biomarker-based screening enables early detection of AL amyloidosis in intermediate/high-risk MGUS patients. Our study shows that identifying pre-symptomatic AL through biomarker longitudinal monitoring allows early treatment, leading to significant organ function recovery.
Keywords: AL amyloidosis; MGUS; biomarkers; screening.
© 2024 The Author(s). American Journal of Hematology published by Wiley Periodicals LLC.
Conflict of interest statement
SM has received honoraria from Bristol‐Myers Squibb, Sanofi, AMGEN, GSK, Takeda, Pfizer, and Janssen, has served on the advisory boards for Sanofi, Takeda, Bristol‐Myers Squibb, Pfizer, and Janssen; GP received honoraria from Pfizer, Serbia, and Siemens and served on advisory boards Alexion, Argobio, GSK, Janssen, and Prothena. PM has received honoraria from Janssen, Pfizer (also research support), Prothena, and Siemens and served on the advisory board for Siemens. LA received honoraria from EUSA Pharma, and Novartis, and served on advisory boards and consultations from Roche, incite, EUSA Pharma, Kite/Gilead, Novartis, and Morphosys.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
