

Factors Associated with Unsuccessful Revascularization Surgery in Traumatic Upper-Extremity Amputation
- PMID: 39629265
- PMCID: PMC11596528
- DOI: 10.2106/JBJS.OA.24.00098
Factors Associated with Unsuccessful Revascularization Surgery in Traumatic Upper-Extremity Amputation
Abstract
Background: Microsurgical emergency revascularization surgery for traumatic upper-extremity amputations demands high resource use. Injury details and patient characteristics influence the decision of whether to revascularize or revise an amputation involving the upper extremity. Our aim was to study associations between those factors and unsuccessful revascularization to provide information for clinical decision-making regarding amputation injuries.
Methods: We studied all consecutive patients who had undergone an upper-extremity revascularization at Tampere University Hospital between 2009 and 2019. The primary outcome was the technical success or failure of the operation, which was defined as the survival or non-survival of the amputated tissue. Using logistic regression, we analyzed prognostic factors including age, sex, smoking status, diabetes mellitus, injury mechanism (cut, crush, or avulsion), extent of tissue loss before treatment (number of lost joints), and amputation type (total or subtotal).
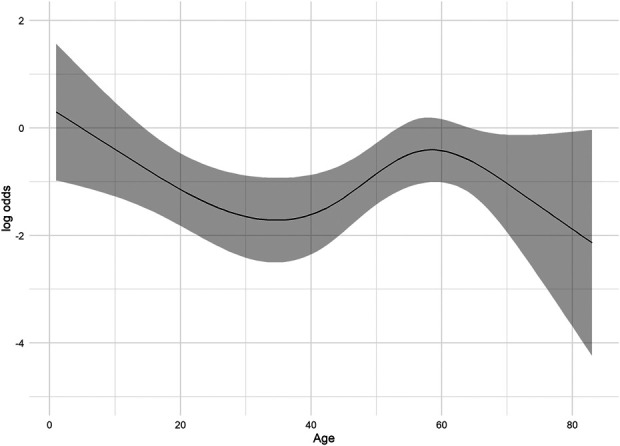
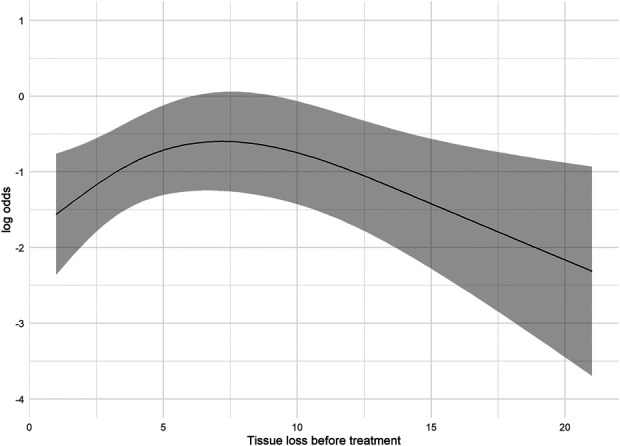
Results: A total of 282 patients (mean age, 47 years; 14% female; mostly White Caucasian) were included. The proportion of successful revascularizations (survival of all reconstructed tissue) was 76% (214 of 282). An avulsion injury mechanism (adjusted odds ratio [aOR], 5.9; 95% confidence interval [CI], 2.5 to 14.2), crush injury mechanism (aOR, 2.8; 95% CI, 1.1 to 7.0]), and total amputation type (aOR, 2.9; 95% CI, 1.5 to 5.8) were the prognostic factors that were associated with the highest risk of unsuccessful revascularizations. We found an S-shaped, nonlinear association between patient age and unsuccessful revascularizations and a U-shaped, nonlinear association between the amount of tissue loss before treatment and unsuccessful revascularizations. There was no evidence of an association between unsuccessful revascularizations and patient sex, smoking, or diabetes mellitus.
Conclusions: Injury details were the most significant prognostic factors of an unsuccessful upper-extremity revascularization, while age was the only patient characteristic that was associated with this outcome. In particular, total amputation type and avulsion and crush injury mechanisms yielded a higher risk of unsuccessful revascularization. We recommend considering this information when making decisions regarding the treatment of upper-extremity amputation injuries.
Level of evidence: Prognostic Level III. See Instructions for Authors for a complete description of levels of evidence.
Copyright © 2024 The Authors. Published by The Journal of Bone and Joint Surgery, Incorporated. All rights reserved.
Conflict of interest statement
Disclosure: No external funding was received for this work. The Disclosure of Potential Conflicts of Interest forms are provided with the online version of the article (http://links.lww.com/JBJSOA/A719).
Figures

References
-
- Lee ZH, Klifto CS, Milone MT, Cohen JM, Daar DA, Anzai L, Thanik VD, Hacquebord JH. Survival after Digit Replantation and Revascularization Is Not Affected by the Use of Interpositional Grafts during Arterial Repair. Plast Reconstr Surg. 2019. Mar;143(3):551e-7e. - PubMed
-
- Yin F, Mi JY, Rui YJ, Xu YJ, Yao Q, Qiu Y, Ke ZS, Sun ZZ. [Risk factors of the failure in digit replantation]. Zhongguo Gu Shang. 2015. May;28(5):429-32. Chinese. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials