

Targeted interferon therapy with modakafusp alfa for relapsed or refractory multiple myeloma
- PMID: 39630057
- PMCID: PMC11969263
- DOI: 10.1182/blood.2024026124
Targeted interferon therapy with modakafusp alfa for relapsed or refractory multiple myeloma
Abstract
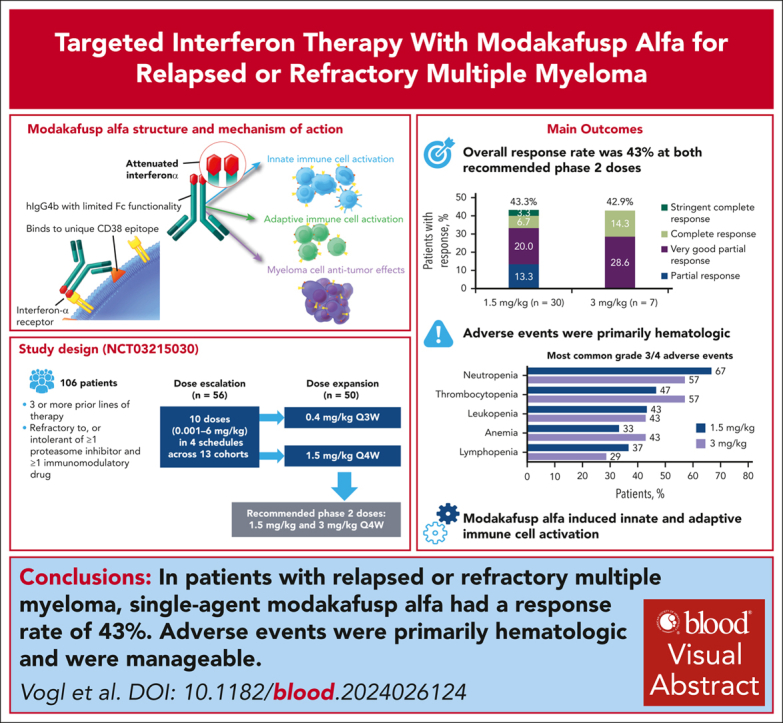
Interferon alfa has activity against multiple myeloma (MM). Modakafusp alfa is an immunocytokine comprising 2 attenuated interferon alfa-2b molecules and an anti-CD38 immunoglobulin G4 antibody, targeting delivery of interferon alfa to CD38-expressing (CD38+) immune and myeloma cells. This phase 1/2 trial enrolled patients with relapsed/refractory multiple myeloma with ≥3 prior lines of treatment and refractory to, or intolerant of, ≥1 proteasome inhibitor and ≥1 immunomodulatory drug. During dose escalation, modakafusp alfa was administered at 10 doses in 4 schedules across 13 cohorts. The primary end point was safety for dose escalation, and overall response rate (ORR) for dose expansion. We enrolled 106 patients who had received a median of 6.5 lines of prior therapy; 84% of patients had myeloma previously refractory to an anti-CD38 antibody. The most feasible dosing schedule was every 4 weeks (Q4W), at which the maximum tolerated dose was 3 mg/kg. Among 30 patients treated at 1.5 mg/kg Q4W, the ORR was 43.3%, with a median duration of response of 15.1 months (95% confidence interval [CI], 7.1-26.1); median progression-free survival was 5.7 months (95% CI, 1.2-14). Grade ≥3 adverse events (AEs) occurred in 28 (93.3%) patients, the most common were neutropenia (66.7%) and thrombocytopenia (46.7%); infections were reported in 8 (26.7%) patients (including grade 3 in 4 [16.7%]). Modakafusp alfa therapy induced upregulation of the type 1 interferon gene signature score, increased CD38 receptor density in CD38+ cells, and innate and adaptive immune cell activation. Modakafusp alfa resulted in antitumor activity and immune activation in patients with MM. AEs were primarily hematologic. This trial was registered at www.clinicaltrials.gov as #NCT03215030.
© 2025 American Society of Hematology. Published by Elsevier Inc. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: D.T.V. reports consulting fees from Takeda, GSK, Genentech, Janssen, Karyopharm, and Oncopeptides; and grants or funds from Takeda and Active Biotech. S.A. reports consulting fees from Janssen and GSK, and grants or funds from Amgen, Janssen, GSK, Bristol Myers Squibb, Karyopharm, and Incyte. S.A.H. reports participation on advisory council or committee for Takeda; consulting fees from AbbVie, Bristol Myers Squibb/Celgene, Janssen, Oncopeptides, Secura Bio, and Takeda; and grants or funds from Bristol Myers Squibb and Oncopeptides. O.N. reports participation on advisory council or committee for Janssen, Bristol Myers Squibb, Karyopharm, Sanofi, Takeda, GPCR Therapeutics, GSK, and Adaptive Biotechnologies; consulting fees from GPCR Therapeutics; and grants or funds from Janssen and Takeda. M.C. reports employment with Bristol Myers Squibb. N.B. reports consulting fees from Janssen, Sanofi, Bristol Myers Squibb, GSK, AbbVie, and Pfizer; and participation in speakers bureau for Janssen. K.S., S.C., and C.L. report employment with and ownership of stocks/shares in Takeda. Y.L. and X.P. report employment with Takeda. X.P. reports owning stock/shares in Takeda. J.L.K. reports consulting fees from Bristol Myers Squibb, Ascentage, Roche, Sanofi, and Sebia. D.B. declares no competing financial interests.
Figures




Comment in
-
Novel interferon-based antimyeloma activity.Blood. 2025 Feb 27;145(9):901-902. doi: 10.1182/blood.2024027417. Blood. 2025. PMID: 40014322 No abstract available.
References
-
- Khoo TL, Vangsted AJ, Joshua D, Gibson J. Interferon-alpha in the treatment of multiple myeloma. Curr Drug Targets. 2011;12(3):437–446. - PubMed
-
- Fritz E, Ludwig H. Interferon-alpha treatment in multiple myeloma: meta-analysis of 30 randomised trials among 3948 patients. Ann Oncol. 2000;11(11):1427–1436. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
