

Risk of Intracranial Hemorrhage Associated With Direct Oral Anticoagulation vs Antiplatelet Therapy: A Systematic Review and Meta-Analysis
- PMID: 39630447
- PMCID: PMC11618459
- DOI: 10.1001/jamanetworkopen.2024.49017
Risk of Intracranial Hemorrhage Associated With Direct Oral Anticoagulation vs Antiplatelet Therapy: A Systematic Review and Meta-Analysis
Abstract
Importance: For patients with atrial fibrillation, clinicians often prescribe antiplatelet therapy rather than oral anticoagulation, which may be related to a concern that direct oral anticoagulants (DOACs) are associated with a higher risk of intracranial bleeding, despite being less effective for stroke prevention.
Objective: To determine whether DOAC therapy, compared with single-agent antiplatelet therapy, was associated with an increased risk of intracranial and major hemorrhage.
Data sources: A systematic search of PubMed and Embase databases from inception to February 7, 2024, was performed.
Study selection: Randomized clinical trials that compared DOAC therapy with single-agent antiplatelet therapies were included. Trials with active follow-up of less than 30 days or a sample size less than 200 were excluded.
Data extraction and synthesis: The study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses reporting guideline. Data were extracted independently by 2 researchers. A random-effects meta-analysis model was used to report pooled treatment effects and 95% CIs.
Main outcomes and measures: The primary outcome was occurrence of intracranial hemorrhage.
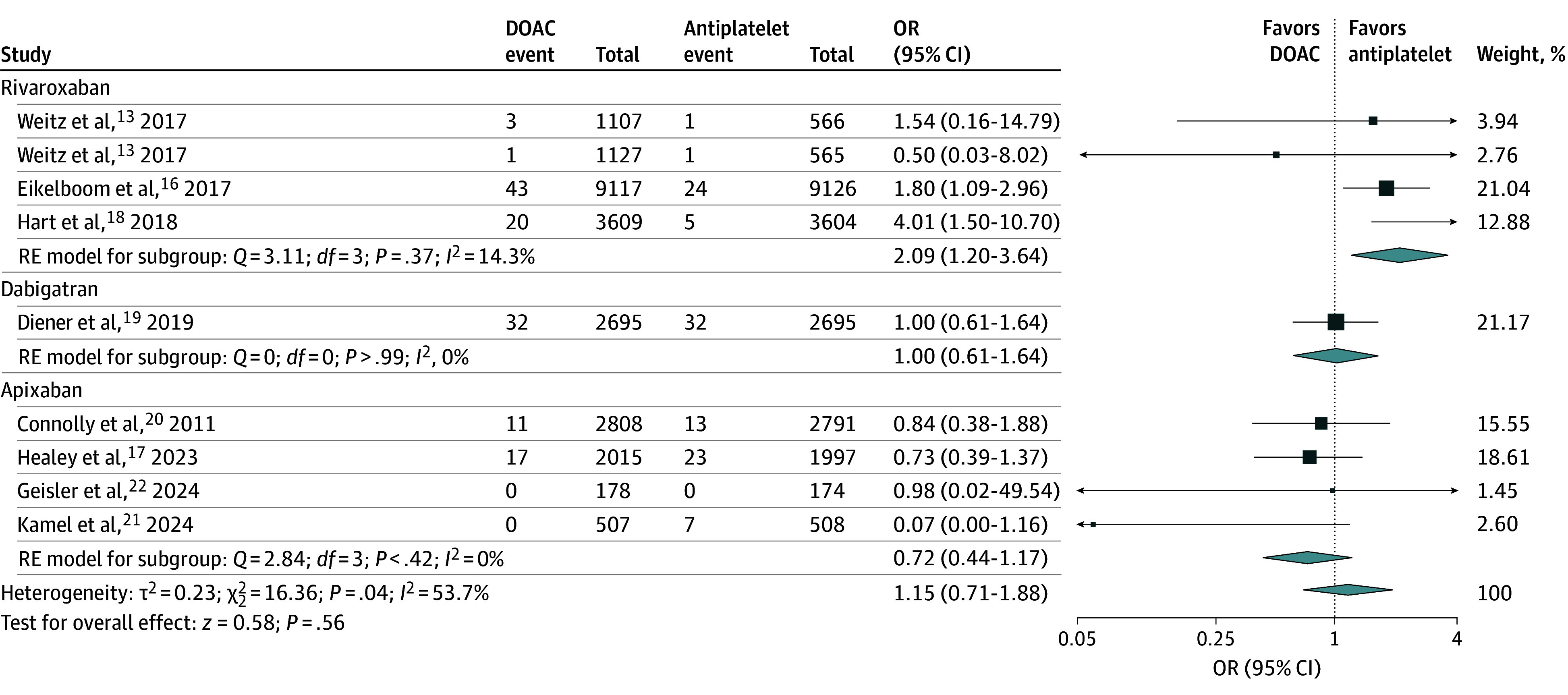
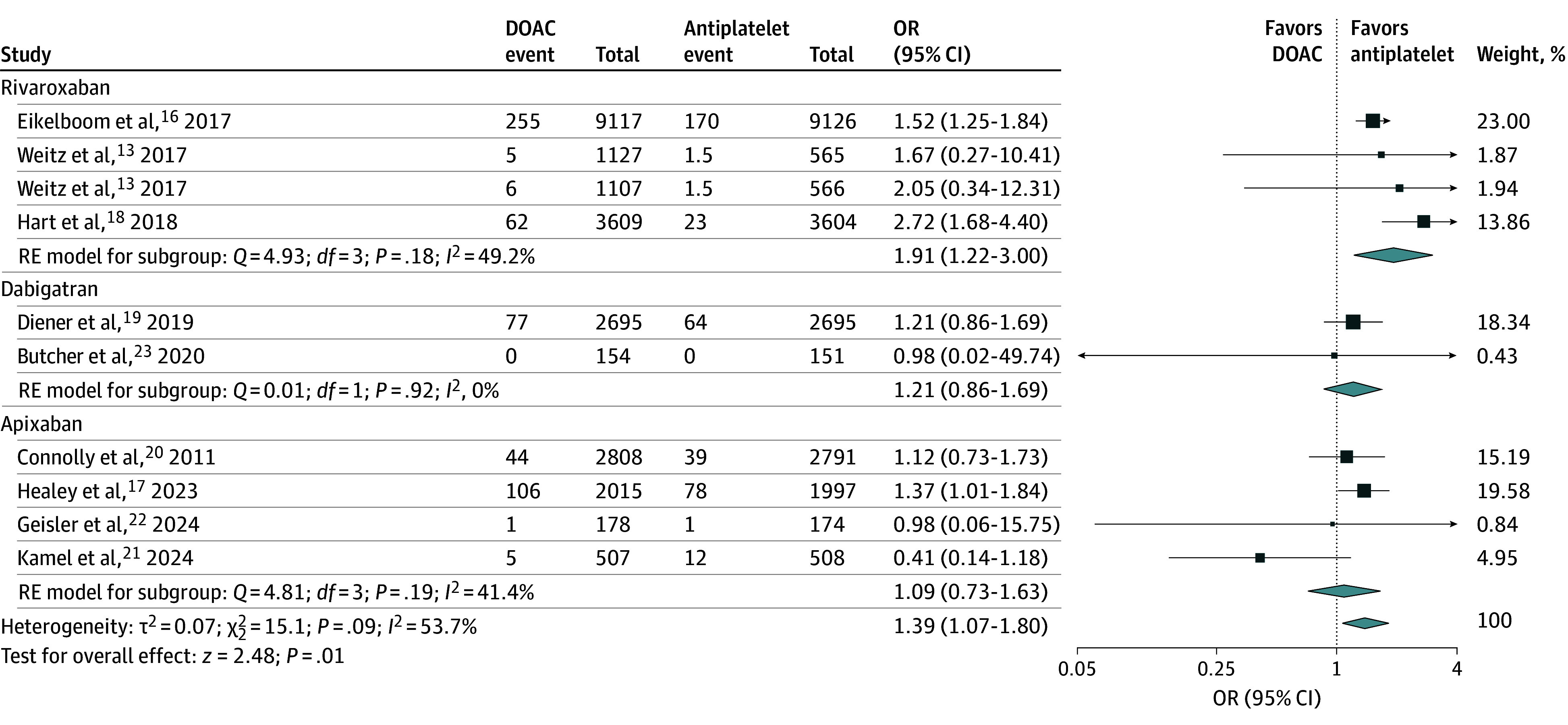
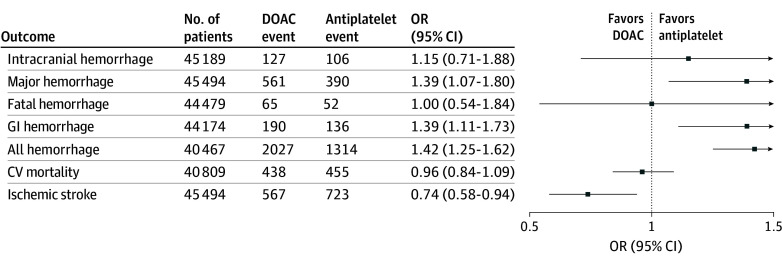
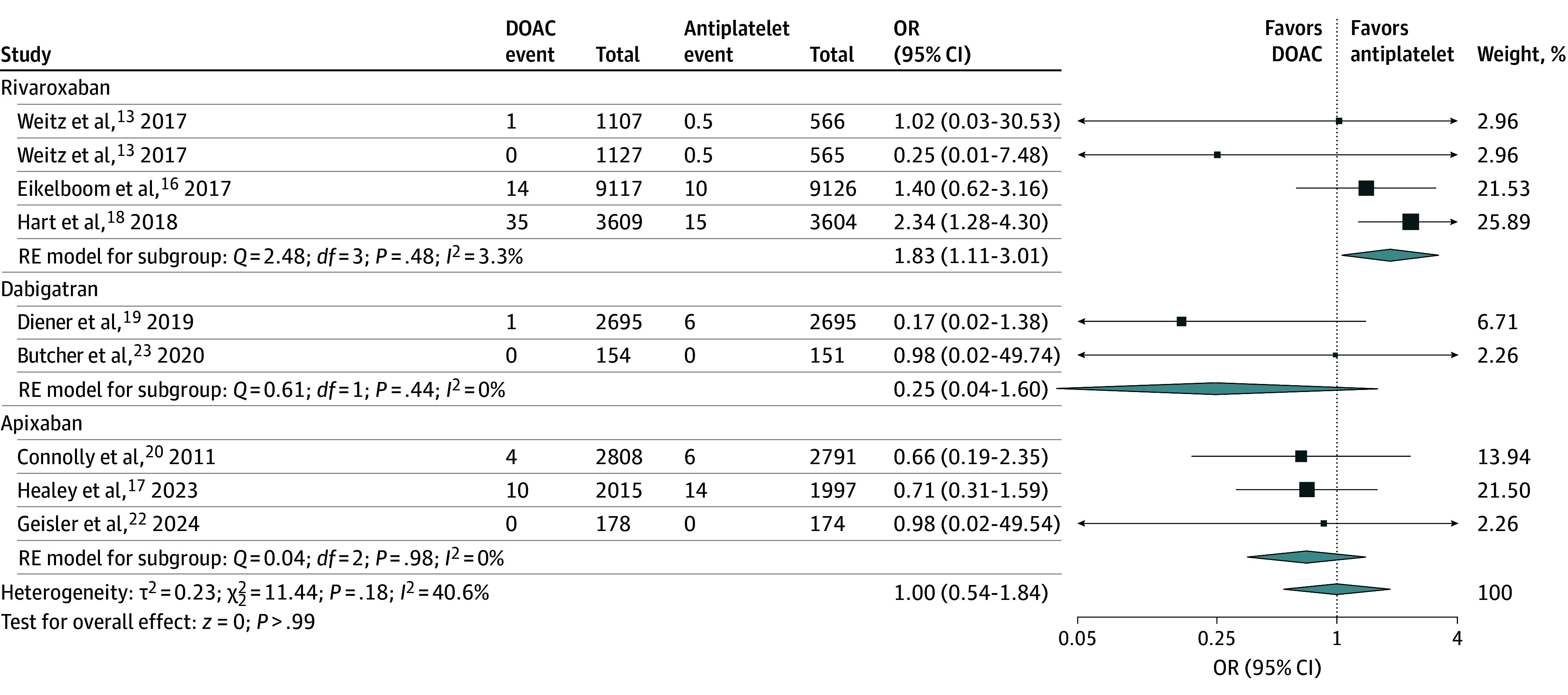
Results: A total of 9 randomized clinical trials were included (45 494 participants). DOAC therapy was not associated with significantly higher odds of intracranial hemorrhage compared with antiplatelet therapy (0.55% vs 0.48% over a mean trial follow-up of 17.1 months; odds ratio [OR], 1.15; 95% CI, 0.71-1.88), but there was heterogeneity among trials (I2 = 53.7%). In an analysis by DOAC agent, the respective estimates for intracranial hemorrhage risk were as follows: rivaroxaban, OR, 2.09 (95% CI, 1.20-3.64); dabigatran, OR, 1.00 (95% CI, 0.61-1.64); and apixaban, OR, 0.72 (95% CI, 0.44-1.17). Overall, DOAC therapy was associated with higher odds of major hemorrhage compared with antiplatelet therapy (2.41% vs 1.76% over a mean trial follow-up of 15.5 months; OR, 1.39; 95% CI, 1.07-1.80), with the following estimates by agent: rivaroxaban, OR, 1.91 (95% CI, 1.22-3.00); dabigatran; OR, 1.21 (95% CI, 0.86-1.69); and apixaban, OR, 1.09 (95% CI, 0.73-1.63).
Conclusions and relevance: In this systematic review and meta-analysis, DOAC therapy was not associated with a significantly higher risk of intracranial hemorrhage compared with antiplatelet therapy, but was associated with a higher risk of major hemorrhage. These findings support the safety of DOAC compared with antiplatelet therapy with respect to risk of ICH and reinforce adherence with current atrial fibrillation guidelines.
Conflict of interest statement
Figures
References
-
- Joglar JA, Chung MK, Armbruster AL, et al. . 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024;149(1):e1-e156. doi:10.1161/CIR.0000000000001193 - DOI - PMC - PubMed
-
- Hindricks G, Potpara T, Dagres N, et al. ; ESC Scientific Document Group . 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373-498. doi:10.1093/eurheartj/ehaa612 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
