

Diverse NKT cells regulate early inflammation and neurological outcomes after cardiac arrest and resuscitation
- PMID: 39630883
- PMCID: PMC11792709
- DOI: 10.1126/scitranslmed.adq5796
Diverse NKT cells regulate early inflammation and neurological outcomes after cardiac arrest and resuscitation
Abstract
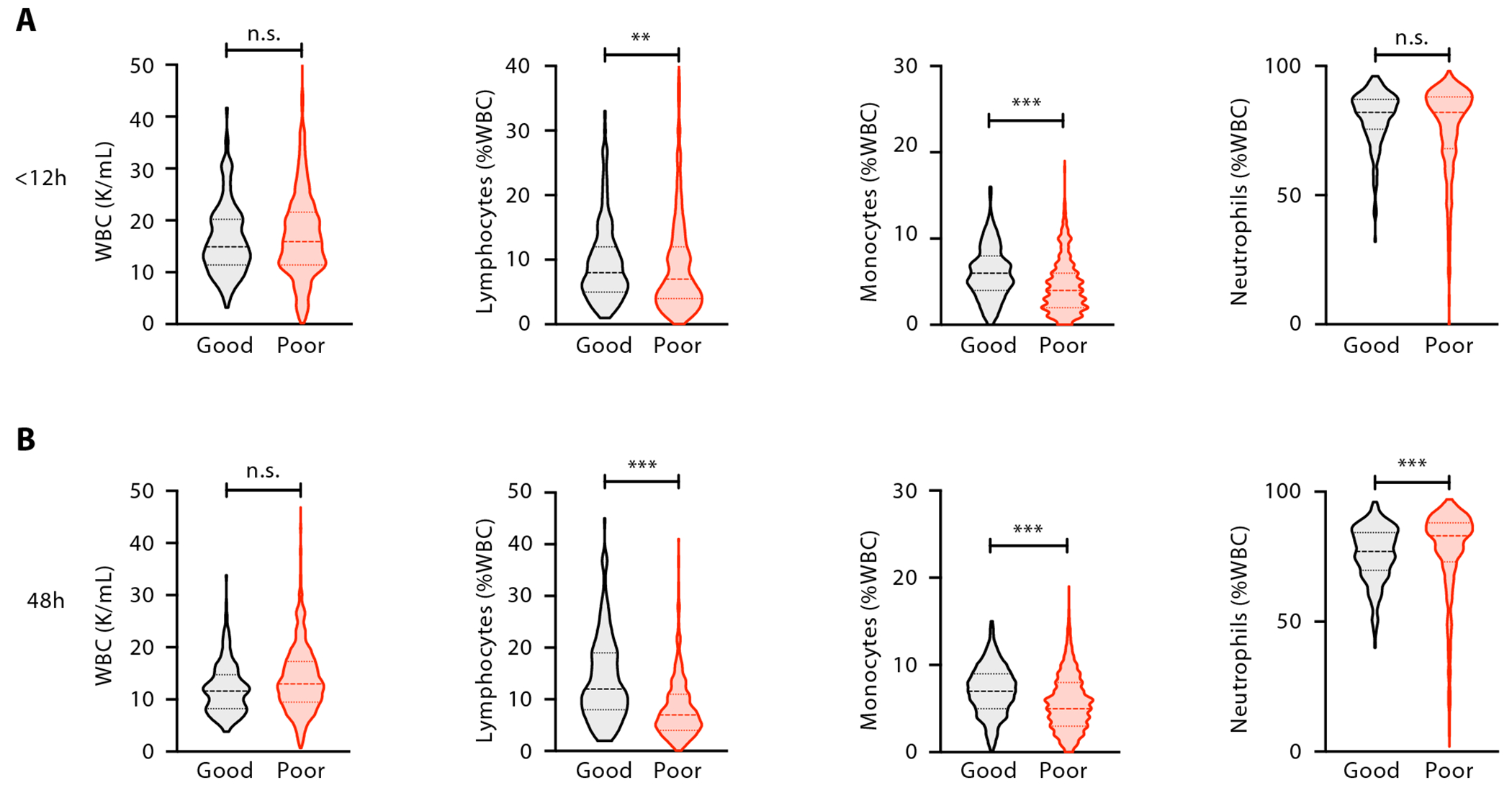
Neurological injury drives most deaths and morbidity among patients hospitalized for out-of-hospital cardiac arrest (OHCA). Despite its clinical importance, there are no effective pharmacological therapies targeting post-cardiac arrest (CA) neurological injury. Here, we analyzed circulating immune cells from a large cohort of patients with OHCA, finding that lymphopenia independently associated with poor neurological outcomes. Single-cell RNA sequencing of immune cells showed that T cells with features of both innate T cells and natural killer (NK) cells were increased in patients with favorable neurological outcomes. We more specifically identified an early increase in circulating diverse NKT (dNKT) cells in a separate cohort of patients with OHCA who had good neurological outcomes. These cells harbored a diverse T cell receptor repertoire but were consistently specific for sulfatide antigen. In mice, we found that sulfatide-specific dNKT cells trafficked to the brain after CA and resuscitation. In the brains of mice lacking NKT cells (Cd1d-/-), we observed increased inflammatory chemokine and cytokine expression and accumulation of macrophages when compared with wild-type mice. Cd1d-/- mice also had increased neuronal injury, neurological dysfunction, and worse mortality after CA. To therapeutically enhance dNKT cell activity, we treated mice with sulfatide lipid after CA, showing that it improved neurological function. Together, these data show that sulfatide-specific dNKT cells are associated with good neurological outcomes after clinical OHCA and are neuroprotective in mice after CA. Strategies to enhance the number or function of dNKT cells may thus represent a treatment approach for CA.
Conflict of interest statement
In disclosures unrelated to this work, RMB serves on Advisory Boards for Merck and Genentech. For disclosure unrelated to this work, PCH owns equity in and serve as consultant for iDoc Telehealth Solutions, Inc. and receives unrelated research funding from National Institute of Health/National Library of Medicine, Center for Disease Control and Prevention, and Day Zero Diagnostics, Inc. DAM and EAB are members of the TIMI Study Group which has received institutional research grant support through Brigham and Women’s Hospital from: Abbott Laboratories, Amgen, Anthos Therapeutics, Arca Biopharma, AstraZeneca, Bayer HealthCare Pharmaceuticals, Inc., Daiichi-Sankyo, Eisai, Intarcia, Janssen, Merck, Novartis, Pfizer, Quark Pharmaceuticals, Regeneron, Roche, Siemens, and Zora Biosciences. DAM has received consulting fees from Abbott Laboratories, InCarda, Inflammatix, Merck, Novartis, Regeneron and Roche Diagnostics. AJW receives research funding unrelated to this work from the National Institutes of Health (NHLBI, NINDS), Society for Academic Emergency Medicine Foundation, Zoll Foundation, National Aeronautics and Space Administration/Translational Research Institute for Space Health, Department of Defense, and the Centers for Disease Control and Prevention. Separately, and also unrelated to this work, AJW has received consulting fees from Inflammatix Inc. FI receives unrelated research funding from Kyowa Hakko Bio and Cyclerion. FI is a member of the Advisory Board of Nihon Kohden Innovation Center and ZOLL foundation Board of Directors. EYK received unrelated research funding from Bayer AG and 10X Genomics. EYK has an unrelated financial interest in Novartis AG. The remaining authors have no other disclosures or conflicts of interest relevant to this work.
Figures






References
-
- Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, Boehme AK, Buxton AE, Carson AP, Commodore-Mensah Y, Elkind MSV, Evenson KR, Eze-Nliam C, Ferguson JF, Generoso G, Ho JE, Kalani R, Khan SS, Kissela BM, Knutson KL, Levine DA, Lewis TT, Liu J, Loop MS, Ma J, Mussolino ME, Navaneethan SD, Perak AM, Poudel R, Rezk-Hanna M, Roth GA, Schroeder EB, Shah SH, Thacker EL, VanWagner LB, Virani SS, Voecks JH, Wang N-Y, Yaffe K, Martin SS, Heart Disease and Stroke Statistics-2022 Update: A Report From the American Heart Association., Circulation 145, e153–e639 (2022). - PubMed
-
- Nielsen N, Wetterslev J, Cronberg T, Erlinge D, Gasche Y, Hassager C, Horn J, Hovdenes J, Kjaergaard J, Kuiper M, Pellis T, Stammet P, Wanscher M, Wise MP, Åneman A, Al-Subaie N, Boesgaard S, Bro-Jeppesen J, Brunetti I, Bugge JF, Hingston CD, Juffermans NP, Koopmans M, Køber L, Langørgen J, Lilja G, Møller JE, Rundgren M, Rylander C, Smid O, Werer C, Winkel P, Friberg H, TTM Trial Investigators, Targeted temperature management at 33°C versus 36°C after cardiac arrest., N. Engl. J. Med 369, 2197–2206 (2013). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
