

Efficacy and Safety of Sacubitril/Valsartan Versus Amlodipine in Japanese Patients With Essential Hypertension: A Randomized, Multicenter, Open-Label, Noninferiority Study (PARASOL Study)
- PMID: 39632589
- PMCID: PMC11771805
- DOI: 10.1111/jch.14938
Efficacy and Safety of Sacubitril/Valsartan Versus Amlodipine in Japanese Patients With Essential Hypertension: A Randomized, Multicenter, Open-Label, Noninferiority Study (PARASOL Study)
Abstract
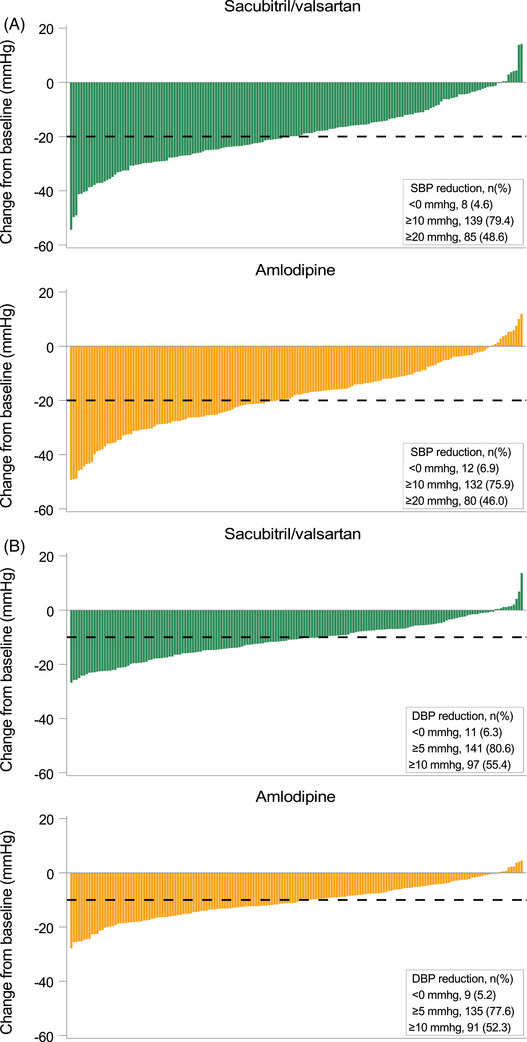
Sacubitril/valsartan, an angiotensin receptor-neprilysin inhibitor, has demonstrated a superior blood pressure-lowering effect compared with renin-angiotensin system inhibitors in several clinical trials. However, there has been no available evidence on the comparison between sacubitril/valsartan and calcium channel blockers (CCBs), a well-established class of antihypertensive drugs. In this open-label, multicenter study, we aimed to demonstrate the efficacy and safety of sacubitril/valsartan versus amlodipine, one of the most widely used CCBs, after 8 weeks of treatment. A total of 359 Japanese patients with essential hypertension (office systolic blood pressure [SBP] ≥ 150 to < 180 mmHg), aged 18-79, were randomly assigned to receive either once-daily sacubitril/valsartan 200 mg or once-daily amlodipine 5 mg in a 1:1 allocation ratio. The primary endpoint was the noninferiority of sacubitril/valsartan compared with amlodipine in mean change in 24-h SBP from baseline to Week 8, followed by a significance test as a secondary endpoint analysis. The mean change in 24-h SBP in sacubitril/valsartan was noninferior to that in amlodipine (between-treatment difference -0.62 mmHg [95% confidential interval: -3.23 to 1.98; p = 0.003 for noninferiority; independent t-test with noninferiority margin 3.0 mmHg]), with no significant difference observed (p = 0.637). There was no significant difference in the incidence of adverse events (AEs). These results suggested that the blood pressure-lowering effect of sacubitril/valsartan is comparable to that of amlodipine, with no marked differences in tolerability between the two groups. Sacubitril/valsartan, a potent antihypertensive drug comparable to amlodipine, is expected to improve blood pressure control in clinical practice.
Keywords: ambulatory blood pressure monitoring; angiotensin receptor‐neprilysin inhibitor; calcium channel blocker; essential hypertension; sacubitril/valsartan.
© 2024 The Author(s). The Journal of Clinical Hypertension published by Wiley Periodicals LLC.
Conflict of interest statement
H.R. has received honoraria from Novartis Pharma K.K., Otsuka Pharmaceutical Co. Ltd., Daiichi Sankyo Co. Ltd., and Takeda Pharmaceutical Co. Ltd.; received research funding from Novartis Pharma K.K.; and has received a scholarship or donation from Daiichi Sankyo Co. Ltd., Kyowa Kirin Co. Ltd., Nippon Boehringer Ingelheim Co. Ltd., Sumitomo Pharma Co. Ltd., and Takeda Pharmaceutical Co. Ltd. K.K. has received honoraria from Omron Healthcare Co. Ltd., CureApp, Inc., Daiichi Sankyo Co. Ltd., Otsuka Pharmaceutical Co. Ltd., Terumo Corporation, Bayer, Kyowa Kirin Co. Ltd., Viatris Pharmaceuticals Japan Inc., and Novartis Pharma K.K.; received research funding from Omron Healthcare Co. Ltd., Fukuda Denshi Co. Ltd., and Edwards Lifesciences Corporation; and has received a scholarship or donation from Otsuka Pharmaceutical Co. Ltd., Daiichi Sankyo Co. Ltd., Nippon Boehringer Ingelheim Co. Ltd., and Sumitomo Pharma Co. Ltd. K.Y. has received honoraria from Daiichi Sankyo Co. Ltd. and Otsuka Pharmaceutical Co. Ltd.; received research funding from Novartis Pharma K.K. and has received a scholarship or donation from Nippon Boehringer Ingelheim Co. Ltd. and Sumitomo Pharma Co. Ltd. D.Y., A.S., S.E., and K.I. are employees of Novartis Pharma K.K. The remaining authors have nothing to disclose.
Figures


References
-
- World Health Organization . Global Report on Hypertension: The Race Against a Silent Killer (Geneva, Switzerland, 2023): 10, https://www.who.int/publications/i/item/9789240081062.
-
- Umemura S., Arima H., Arima S., et al., “The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019),” Hypertension Research 42 (2019): 1235–1481. - PubMed
-
- Mancia G., Kreutz R., Brunström M., et al., “2023 ESH Guidelines for the Management of Arterial Hypertension The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA),” Journal of Hypertension 41 (2023): 1874–2071. - PubMed
-
- Ruilope L. M., Dukat A., Böhm M., et al., “Blood‐Pressure Reduction With LCZ696, a Novel Dual‐Acting Inhibitor of the Angiotensin II Receptor and Neprilysin: A Randomised, Double‐Blind, Placebo‐Controlled, Active Comparator Study,” Lancet 375 (2010): 1255–1266. - PubMed
-
- Jhund P. S., Claggett B., Packer M., et al., “Independence of the Blood Pressure Lowering Effect and Efficacy of the Angiotensin Receptor Neprilysin Inhibitor, LCZ696, in Patients With Heart Failure With Preserved Ejection Fraction: An Analysis of the PARAMOUNT Trial,” European Journal of Heart Failure 16 (2014): 671–677. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
