

Sex differences in the association of dietary inflammatory index with chronic kidney disease in US adults
- PMID: 39632932
- PMCID: PMC11618389
- DOI: 10.1038/s41598-024-78307-4
Sex differences in the association of dietary inflammatory index with chronic kidney disease in US adults
Abstract
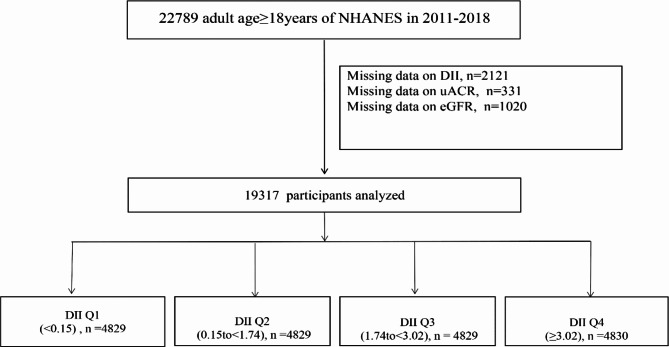
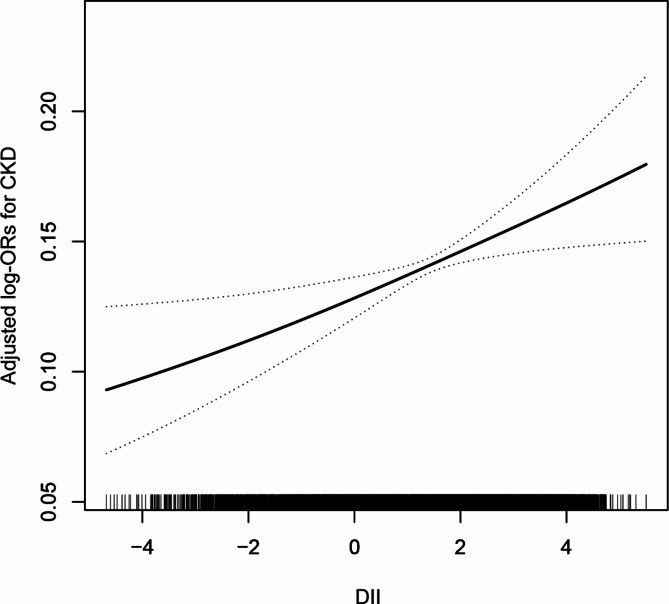
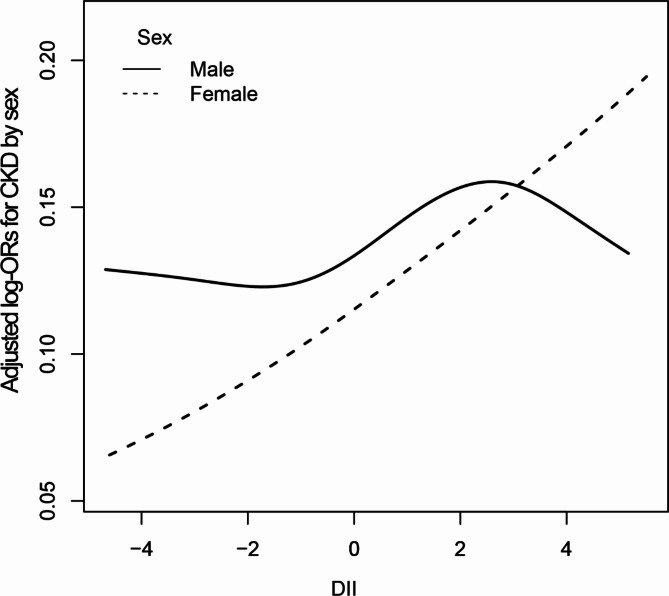
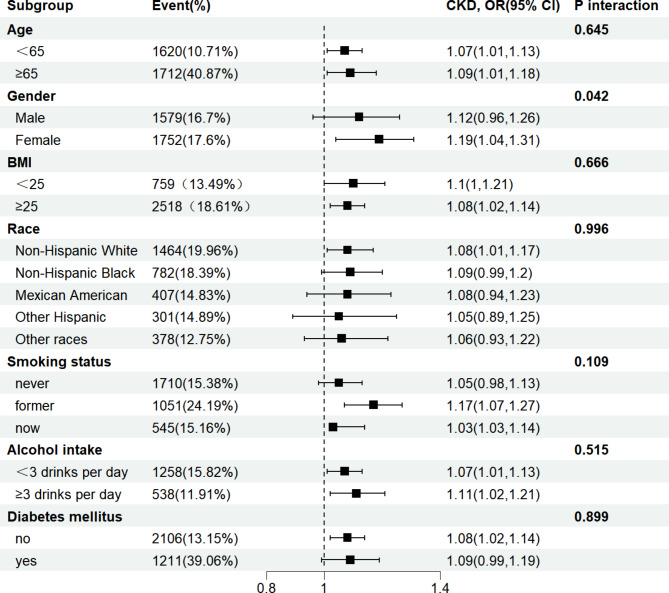
Studies on the association between dietary inflammatory index (DII) and chronic kidney disease (CKD) are limited. We aimed to examine the association between DII and CKD among U.S. adults with particular attention paid to sex differences. A total of 19317participants were included in this study. The exposure variable was DII, which was calculated based on overall inflammatory effect scores. The outcome was CKD, defined as estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m2 or urinary albumin/creatinine (uACR) ≥ 30 mg/g. The mean (SD) of age our study participants was 47.84 (18.35); and the mean (SD) of DII was 1.50 (1.91) (median 1.74). In multivariate logistic regression analysis, we observed that the OR value (95%CI) of CKD is 1.19 (1.14, 1.23), 1.12 (1.06, 1.19), and 1.16 (1.06, 1.27) in models 1, 2 and 3 for Per SD increment of DII. Compared with Participants with Q1(DII < 0.15), the adjusted ORs for participants in Q2 (0.15 ≤ DII < 1.74), Q3 (1.74 ≤ DII < 3.02) and Q4 (≥ 3.02)were 1.46 (95% CI 1.14-1.88), 1.55 (95% CI 1.20-1.99) and 1.52 (95% CI 1.17, 1.98) ( p for trend < 0.05), respectively. However, this study observed that the independent positive correlation between DII and CKD appeared in women rather than men. Higher DII levels were significantly and linearly associated with an increased prevalence of chronic kidney disease, and sex modified the association. This suggests that gender-specific dietary interventions can be developed to reduce the risk of CKD.
Keywords: Chronic kidney disease; Dietary inflammatory index; Females; Sex differences.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethical approval and consent to participate: All procedures performed in studies involving human participants were following the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All participants provided written informed consent. And this survey was approved by the Ethics Review Board of the National Center for Health Statistics. Informed consent: Informed consent was obtained from all individual participants included in the study.
Figures
Similar articles
-
Associations of dietary inflammatory index with low estimated glomerular filtration rate, albuminuria and chronic kidney disease in U.S adults: Results from the NHANES 2011-2018.Nutr Metab Cardiovasc Dis. 2024 Apr;34(4):1036-1045. doi: 10.1016/j.numecd.2023.11.006. Epub 2023 Dec 1. Nutr Metab Cardiovasc Dis. 2024. PMID: 38267324
-
Greater Dietary Inflammatory Index score is associated with higher likelihood of chronic kidney disease.Br J Nutr. 2018 Jul;120(2):204-209. doi: 10.1017/S0007114518001071. Br J Nutr. 2018. PMID: 29947319
-
Higher Dietary Inflammatory Index and Systemic Immune-Inflammation Index Score are Associated With Higher Risk of Chronic Kidney Disease: Analysis of the National Health and Nutrition Examination Survey From 1999 to 2018.J Ren Nutr. 2025 Mar;35(2):300-310. doi: 10.1053/j.jrn.2024.07.013. Epub 2024 Jul 27. J Ren Nutr. 2025. PMID: 39074600
-
Association of Chronic Kidney Disease With Dietary Inflammatory Index in Adults Aged 50 Years and Older: Dose-Response Analysis of a Nationally Representative Population-Based Study.J Ren Nutr. 2024 May;34(3):216-222. doi: 10.1053/j.jrn.2023.09.007. Epub 2023 Oct 5. J Ren Nutr. 2024. PMID: 37805190
-
Association of Dietary Inflammatory Index with CKD progression and estimated glomerular filtration rate in the American CKD population: A cross-sectional study.PLoS One. 2024 Feb 22;19(2):e0297916. doi: 10.1371/journal.pone.0297916. eCollection 2024. PLoS One. 2024. PMID: 38386646 Free PMC article.
Cited by
-
Association between dietary inflammatory index score and cardiovascular-kidney-metabolic syndrome: a cross-sectional study based on NHANES.Front Nutr. 2025 May 9;12:1557491. doi: 10.3389/fnut.2025.1557491. eCollection 2025. Front Nutr. 2025. PMID: 40416382 Free PMC article.
-
Sex-Specific Biochemical and Histopathological Effects of Chronic Meat-Based vs. Plant-Based Burger Consumption in a Rodent Model.Foods. 2025 Mar 5;14(5):888. doi: 10.3390/foods14050888. Foods. 2025. PMID: 40077591 Free PMC article.
References
-
- El Minshawy, O., Ghabrah, T. & El Bassuoni, E. Diabetic nephropathy as a cause of end-stage renal disease in Tabuk area, Saudi Arabia: a four-year study. Saudi J. Kidney Dis. Transpl.25, 1105–1109. 10.4103/1319-2442.139967 (2014). - PubMed
-
- Miyamoto, T., Carrero, J. J. & Stenvinkel, P. Inflammation as a risk factor and target for therapy in chronic kidney disease. Curr. Opin. Nephrol. Hypertens.20, 662–668. 10.1097/MNH.0b013e32834ad504 (2011). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
