

Dichotomous horizontal representation of acute deterioration risk on illnesses
- PMID: 39632948
- PMCID: PMC11618330
- DOI: 10.1038/s41598-024-81592-8
Dichotomous horizontal representation of acute deterioration risk on illnesses
Abstract
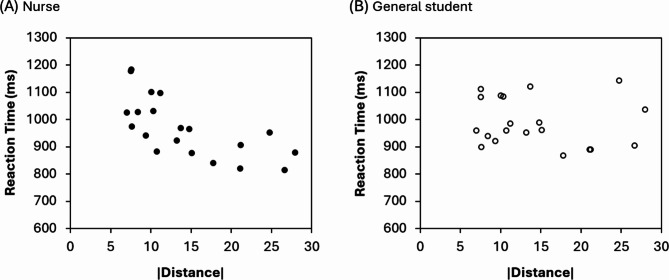
The possibility that risks interact with spatial information (such as the SNARC effect) has been explored but studies did not demonstrate a consistent left-to-right representation of risks. This is probably due to the perception of risk being different in each individual experience. The present study aimed to clarify the spatial characteristics of acute deterioration risks perceived from illnesses. Registered nurses and general students participated in the present experiment. They were instructed to judge, by pressing one of the left/right response buttons, whether the risk of a given target (illness name) presented on a computer screen was higher or lower compared to that of a standard stimulus. Reaction times to the target were measured. No spatial-risk association was observed in the comprehensive analysis, but further inspection revealed that approximately half of the participants have a left-to-right representation and the other half have a right-to-left representation. Moreover, participants' responses appeared to be faster when the target was representationally farther away from the standard stimulus (i.e., distance effect). These findings therefore suggest a spatially aligned magnitude representation of acute deterioration risk (i.e., mental risk line) but this horizontal risk orientation is likely to be dichotomous depending on the individuals and/or given situations.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethical approval: This study was approved by the Research Ethics Committee of Tokyo Metropolitan University Minami-Osawa Campus (Approval number: H5-78 and H6-114). All participants were informed of the study procedure and signed the written informed consent form before participating in the study. Additionally, the study was conducted in accordance with the Declaration of Helsinki.
Figures




References
-
- Dehaene, S., Bossini, S. & Giraux, P. The mental representation of parity and number magnitude. J. Exp. Psychol. Gen.122, 371–396 (1993). - DOI
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
