

Monocyte to high-density lipoprotein cholesterol ratio predicts restenosis of drug-eluting stents in patients with unstable angina pectoris
- PMID: 39632977
- PMCID: PMC11618658
- DOI: 10.1038/s41598-024-81818-9
Monocyte to high-density lipoprotein cholesterol ratio predicts restenosis of drug-eluting stents in patients with unstable angina pectoris
Abstract
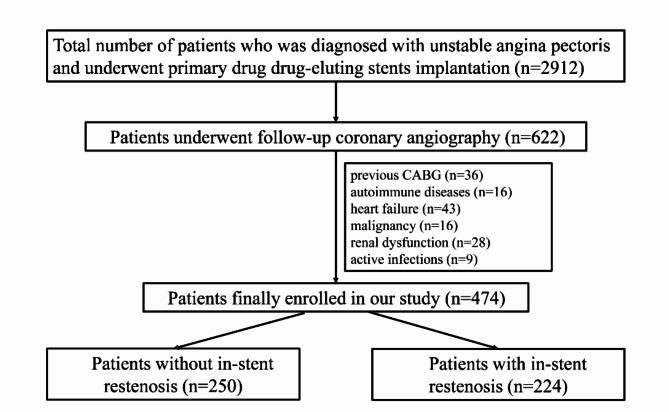
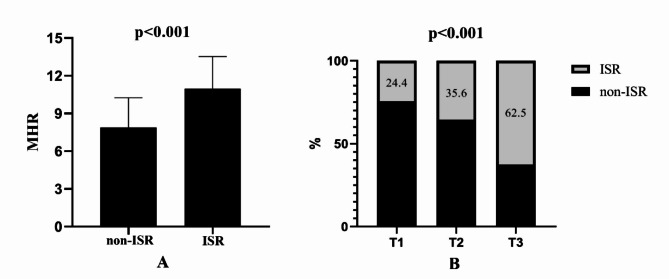
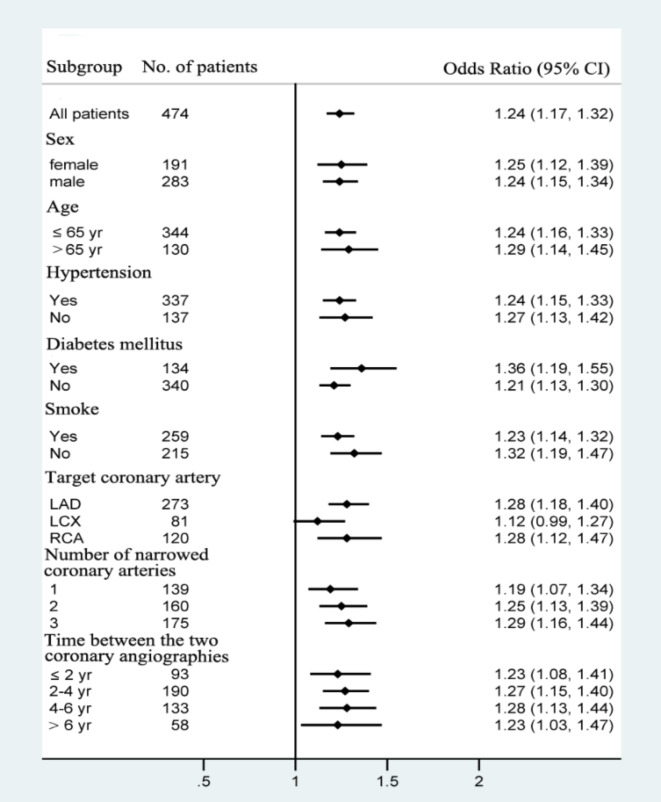
Several studies have shown that the monocyte count to high-density lipoprotein cholesterol ratio (MHR) serves as a predictive marker for in-stent restenosis (ISR) of bare-metal stents (BMSs). However, the ability of the MHR to predict ISR in patients with drug-eluting stents (DESs) remains uncertain. This study aimed to investigate the predictive value of the MHR for ISR in patients with unstable angina pectoris who have undergone primary DES implantation. A total of 474 consecutive patients with unstable angina pectoris who underwent successful DES-based percutaneous coronary intervention (PCI) from 01-12-2014 to 01-12-2022 were enrolled in the study. Patients were divided into the ISR group and the non-ISR group on the basis of the follow-up results of coronary angiography. The demographic and clinical characteristics of the patients were documented. The MHR was calculated via the following formula: [Formula: see text]. Multivariate logistic regression models were developed to evaluate the predictive value of the MHR for DES-ISR. The baseline MHR was notably greater in the ISR group than in the non-ISR group (P < 0.001). After adjusting for confounding factors, the MHR emerged as an independent predictor of ISR (OR = 1.244; 95%CI 1.171-1.321). Receiver operating characteristic (ROC) curve analysis revealed that MHR for predicting ISR had an AUC of 0.752 (95% CI 0.708-0.796). For a MHR > 7.32, the sensitivity was estimated to be 59.8% (95% CI 47.2-66.5%) and the specificity was 81.2% (95% CI 71.2-86.4%). Including the MHR in the predictive model for ISR improved the area under the curve (0.698 vs. 0.782, P < 0.001), categorical net reclassification improvement (0.703; 95%CI 0.536-0.871), and integrated discrimination improvement (0.121; 95%CI 0.092-0.151). The MHR can be used to predict DES-ISR in patients with unstable angina pectoris, indicating that the MHR may serve as a valuable marker for risk stratification and prognosis in individuals undergoing DES implantation.
Keywords: Biomarker; Drug-eluting stent; In-stent restenosis; Monocyte-to-high-density lipoprotein cholesterol ratio; Percutaneous coronary intervention; Unstable angina pectoris.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethical approval and consent to participate: This study was submitted to and approved by the Ethics Commission of Chest Hospital, Tianjin University (IRB-SOP-016[F]-001-03), and strictly adhered to the principles of the Declaration of Helsinki. This was a retrospective study, so the content to be included was not applicable. Consent for publication: This study does not contain data from any individual person, so consent for publication is not applicable.
Figures

References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
