

Evolution of myeloid-mediated immunotherapy resistance in prostate cancer
- PMID: 39633050
- PMCID: PMC11779626
- DOI: 10.1038/s41586-024-08290-3
Evolution of myeloid-mediated immunotherapy resistance in prostate cancer
Abstract
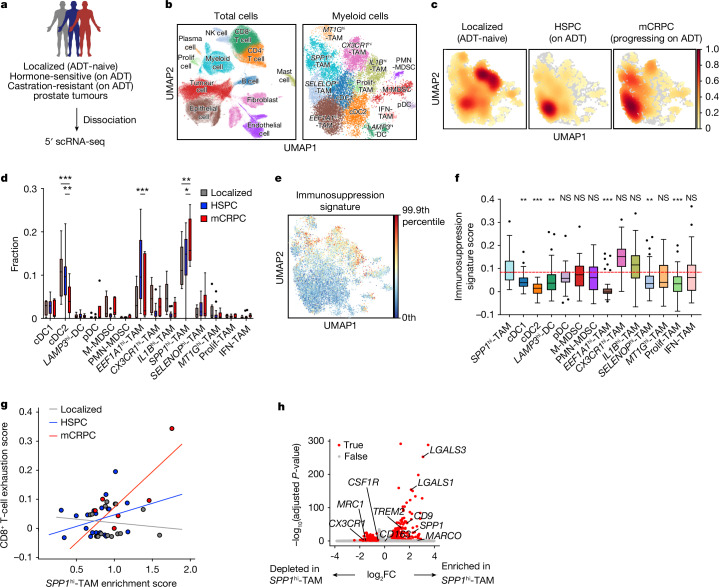
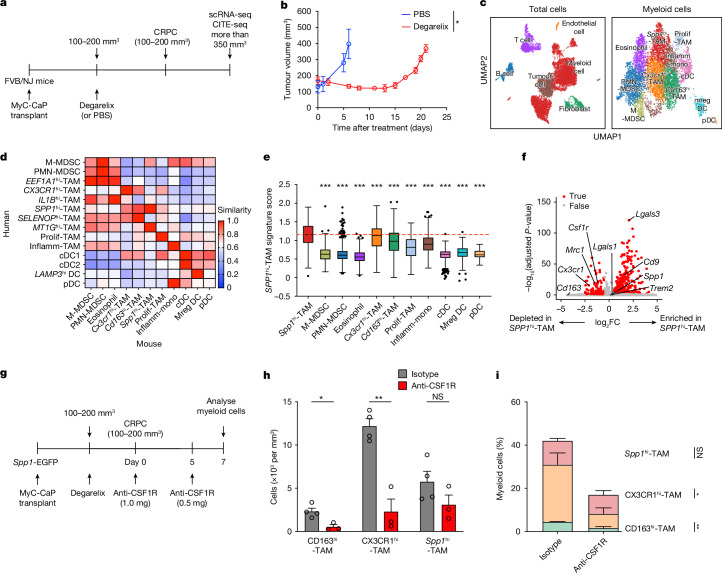
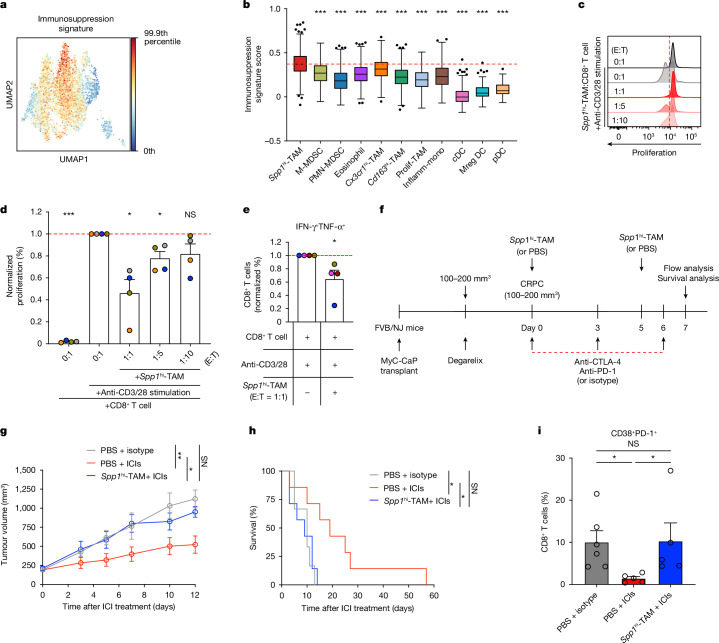
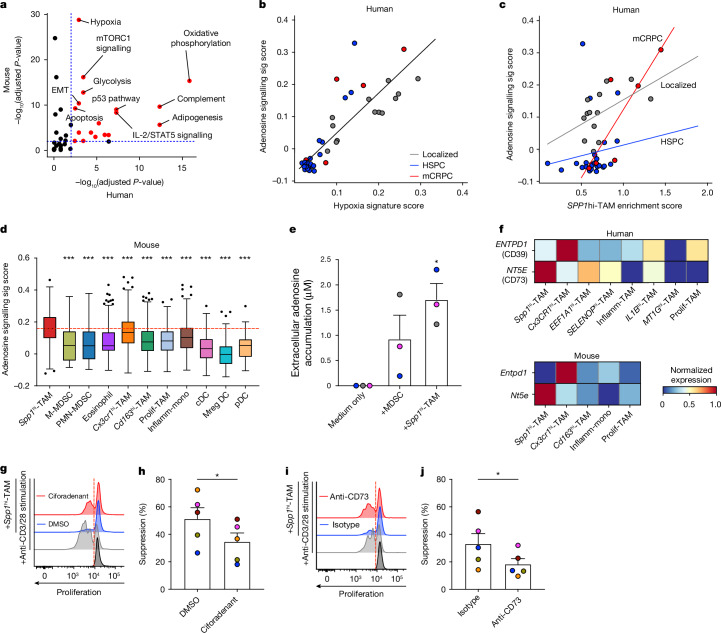
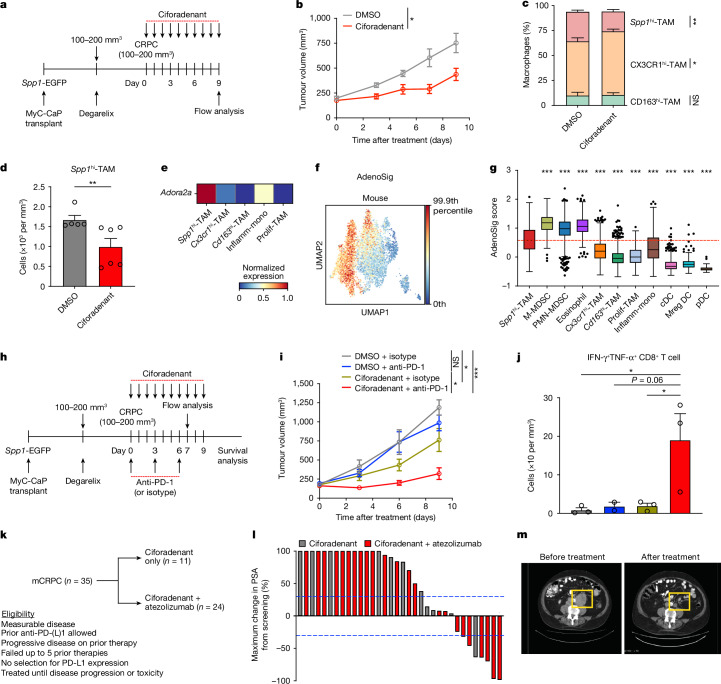
Patients with advanced metastatic castration-resistant prostate cancer (mCRPC) are refractory to immune checkpoint inhibitors (ICIs)1,2, partly because there are immunosuppressive myeloid cells in tumours3,4. However, the heterogeneity of myeloid cells has made them difficult to target, making blockade of the colony stimulating factor-1 receptor (CSF1R) clinically ineffective. Here we use single-cell profiling on patient biopsies across the disease continuum and find that a distinct population of tumour-associated macrophages with elevated levels of SPP1 transcripts (SPP1hi-TAMs) becomes enriched with the progression of prostate cancer to mCRPC. In syngeneic mouse modelling, an analogous macrophage population suppresses CD8+ T cell activity in vitro and promotes ICI resistance in vivo. Furthermore, Spp1hi-TAMs are not responsive to anti-CSF1R antibody treatment. Pathway analysis identifies adenosine signalling as a potential mechanism for SPP1hi-TAM-mediated immunotherapeutic resistance. Indeed, pharmacological inhibition of adenosine A2A receptors (A2ARs) significantly reverses Spp1hi-TAM-mediated immunosuppression in CD8+ T cells in vitro and enhances CRPC responsiveness to programmed cell death protein 1 (PD-1) blockade in vivo. Consistent with preclinical results, inhibition of A2ARs using ciforadenant in combination with programmed death 1 ligand 1 (PD-L1) blockade using atezolizumab induces clinical responses in patients with mCRPC. Moreover, inhibiting A2ARs results in a significant decrease in SPP1hi-TAM abundance in CRPC, indicating that this pathway is involved in both induction and downstream immunosuppression. Collectively, these findings establish SPP1hi-TAMs as key mediators of ICI resistance in mCRPC through adenosine signalling, emphasizing their importance as both a therapeutic target and a potential biomarker for predicting treatment efficacy.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: L.F. has received research support from Roche/Genentech, Abbvie, Bavarian Nordic, Bristol Myers Squibb, Dendreon, Janssen and Merck; has served on the scientific advisory boards of Actym, Astra Zeneca, Bioatla, Bristol Myers Squibb, Daiichi Sankyo, Immunogenesis, Innovent, Merck, Merck KGA, Nutcracker, RAPT, Senti, Sutro and Roche/Genentech; and reports ownership interest in Actym, BioAtla, ImmunoGenesis, Nutcracker, RAPT, Senti and Therapaint. R.A.M. is an employee of Corvus Pharmaceuticals. E.M.V.A. has received research support from Novartis, BMS and Sanofi, and served on the scientific advisory boards of Tango Therapeutics, Genome Medical, Genomic Life, Enara Bio, Manifold Bio, Monte Rosa, Novartis Institute for Biomedical Research, Riva Therapeutics and Serinus Bio. The remaining authors declare no competing interests.
Figures










Comment in
-
A distinct TAM subset mediates immunotherapy resistance in prostate cancer.Nat Rev Urol. 2025 Feb;22(2):70. doi: 10.1038/s41585-025-00996-x. Nat Rev Urol. 2025. PMID: 39820137 No abstract available.
References
-
- Beer, T. M. et al. Randomized, double-blind, phase III trial of ipilimumab versus placebo in asymptomatic or minimally symptomatic patients with metastatic chemotherapy-naive castration-resistant prostate cancer. J. Clin. Oncol.35, 40–47 (2017). - PubMed
-
- Siegel, R. L., Miller, K. D., Wagle, N. S. & Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin.73, 17–48 (2023). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
