

Risk factors and nomogram for the prediction of intracranial hemorrhage in very preterm infants
- PMID: 39633312
- PMCID: PMC11616105
- DOI: 10.1186/s12887-024-05274-0
Risk factors and nomogram for the prediction of intracranial hemorrhage in very preterm infants
Abstract
Aims: This study aims to identify important risk factors for intracranial hemorrhage (ICH) in very preterm infants at our institution and develop a predictive nomogram for early detection of ICH.
Methods: We retrospectively analyzed neonates with a gestational age (GA) under 32 weeks, admitted to the neonatal intensive care unit from March 2022 to July 2023. Infants were categorized into two groups based on ultrasound findings and assessed for thirteen variables including gender, GA, birth weight (BW), acidosis, among others. We used multivariate logistic regression analysis to build a prediction model and identify independent risk factors for ICH. We build a prediction model by assigning 241 cases to the training set and 103 to the validation set (ratio 7:3).
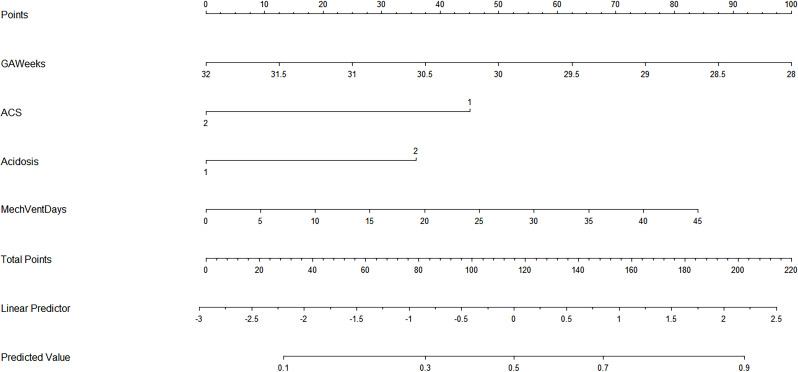
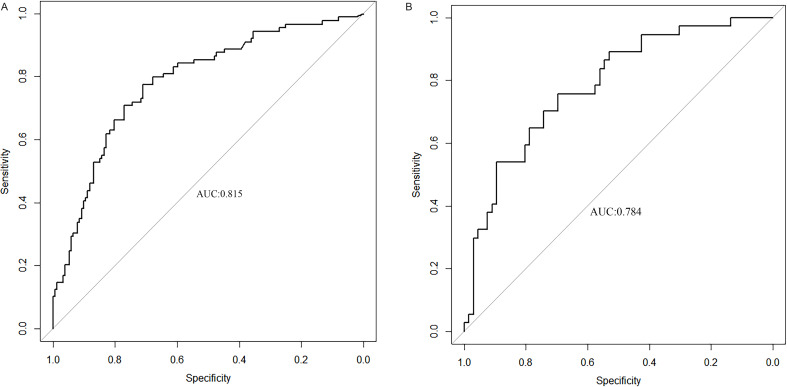
Results: Among 344 very preterm infants, the incidence of ICH was 36.9% (89 cases) in training set. Significant differences were observed in gestational age, birth weight, antenatal corticosteroids, mechanical ventilation days, and acidosis between cases and controls. Logistic regression analysis identified gestational age (OR = 0.674), antenatal corticosteroids (OR = 0.257), acidosis (OR = 2.556), and mechanical ventilation mechanical ventilation days(OR = 0.257) as independent risk factors for ICH. The C-index of the training and validation sets was 0.814 (95% CI: 0.762-0.869) and 0.784 (95% CI: 0.693-0.875), respectively. According to decision curve analysis, our model outperformed the "None" and "All" baseline lines over a wide range of risk thresholds (0.12-0.92).
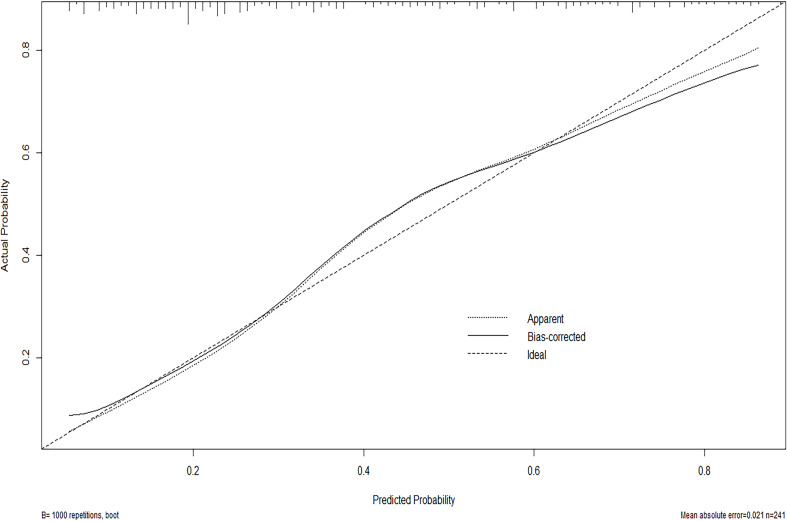
Conclusion: Acidosis and mechanical ventilation are independent risk factors for ICH in very preterm neonates, while higher gestational age and antenatal corticosteroid use are protective. The nomogram developed from these four factors demonstrates strong predictive accuracy and calibration, which can aid clinicians in identifying preterm infants at high risk for ICH and facilitate early diagnosis and management.
Keywords: Intracranial hemorrhage; Nomogram; Prediction model; Risk factors; Very preterm neonates.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Dongguan Maternal and Child Health Care Hospital Ethics Committee and was carried out in accordance with the World Medical Association Declaration of Helsinki. All subjects provided written informed consent. Consent for publication: Not applicable. Informed consent: Informed consent was obtained from the parents or legal guardians of all minor participants involved in this study. Competing interests: The authors declare no competing interests.
Figures



Similar articles
-
Establishment and validation of apnea risk prediction models in preterm infants: a retrospective case control study.BMC Pediatr. 2024 Oct 11;24(1):654. doi: 10.1186/s12887-024-05125-y. BMC Pediatr. 2024. PMID: 39394551 Free PMC article.
-
Development and validation of a nomogram to predict intracranial haemorrhage in neonates.Pediatr Neonatol. 2024 Sep;65(5):493-499. doi: 10.1016/j.pedneo.2024.02.005. Epub 2024 Mar 28. Pediatr Neonatol. 2024. PMID: 38627110
-
[Establishment of a predictive nomogram model for predicting the death of very preterm infants during hospitalization].Zhongguo Dang Dai Er Ke Za Zhi. 2022 Jun 15;24(6):654-661. doi: 10.7499/j.issn.1008-8830.2202027. Zhongguo Dang Dai Er Ke Za Zhi. 2022. PMID: 35762432 Free PMC article. Clinical Trial. Chinese.
-
Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993-2012.JAMA. 2015 Sep 8;314(10):1039-51. doi: 10.1001/jama.2015.10244. JAMA. 2015. PMID: 26348753 Free PMC article.
-
Haemophilia in extreme immature preterm infants: increased risk for intracranial haemorrhage?J Matern Fetal Neonatal Med. 2014 Apr;27(6):621-4. doi: 10.3109/14767058.2013.825600. Epub 2013 Aug 20. J Matern Fetal Neonatal Med. 2014. PMID: 23865671 Review.
Cited by
-
Prediction models for intraventricular hemorrhage in very preterm infants: a systematic review.Front Pediatr. 2025 Jun 4;13:1605145. doi: 10.3389/fped.2025.1605145. eCollection 2025. Front Pediatr. 2025. PMID: 40535700 Free PMC article. Review.
References
-
- Starr R, De Jesus O, Shah SD, Borger J, Periventricular. and Intraventricular Hemorrhage. 2023 Aug 23. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. - PubMed
-
- Bowerman RA, Donn SM, Silver TM, Jaffe MH. Natural history of neonatal periventricular/intraventricular hemorrhage and its complications: sonographic observations. AJR Am J Roentgenol. 1984;143(5):1041–52. - PubMed
-
- Starr R, De Jesus O, Shah SD, Borger J. Periventricular And Intraventricular Hemorrhage. StatPearls. 2022, StatPearls Publishing LLC.; 2022. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
