

Posterior iliac crest vs. proximal tibia: distinct sources of anti-inflammatory and regenerative cells with comparable 6-month clinical outcomes in treatment of osteoarthritis
- PMID: 39633422
- PMCID: PMC11616267
- DOI: 10.1186/s12967-024-05924-y
Posterior iliac crest vs. proximal tibia: distinct sources of anti-inflammatory and regenerative cells with comparable 6-month clinical outcomes in treatment of osteoarthritis
Abstract
Background: Human bone marrow is a source of mesenchymal stem cells (MSCs), other progenitor cells, and factors with anti-inflammatory and regenerative capacity. Though the fraction of MSCs out of the nucleated cells is very small, bone marrow aspirate (BMA) for osteoarthritis (OA) has noteworthy effects. BMA is usually collected from the posterior or anterior iliac crest, and rarely from the proximal tibia. We investigated the clinically beneficial concentration of ex vivo MSCs, derived from BM harvested from the posterior iliac crest and proximal tibia by Marrow Cellution™ Aspiration System, and their phenotypic differences, in comparison to autologous Platelet-Rich Plasma (PRP) treatment prepared with a manual, closed system.
Methods: A single-center, parallel, randomized controlled study was designed to investigate the efficacy of BMA from the posterior iliac crest compared to BMA from the proximal tibia, against a control group treated with PRP, in knee OA. Thirty patients with knee OA grade I-IV, according to Kellgren-Lawrence (KL), were distributed into each group. Visual Analog Scale (VAS) and Western Ontario & McMaster Universities Arthritis Index (WOMAC) score were used for clinical outcome evaluation.
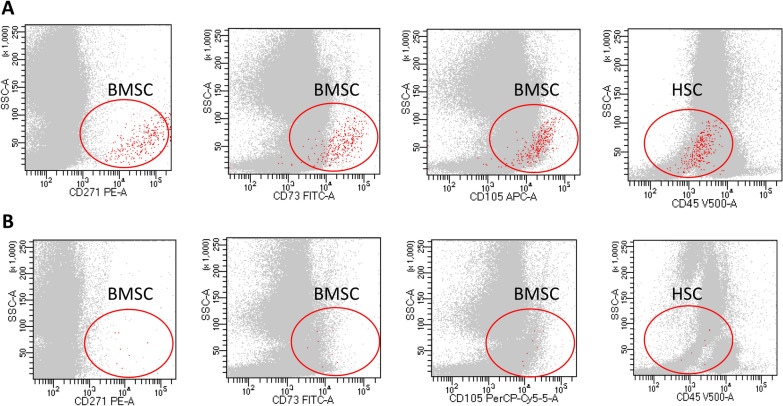
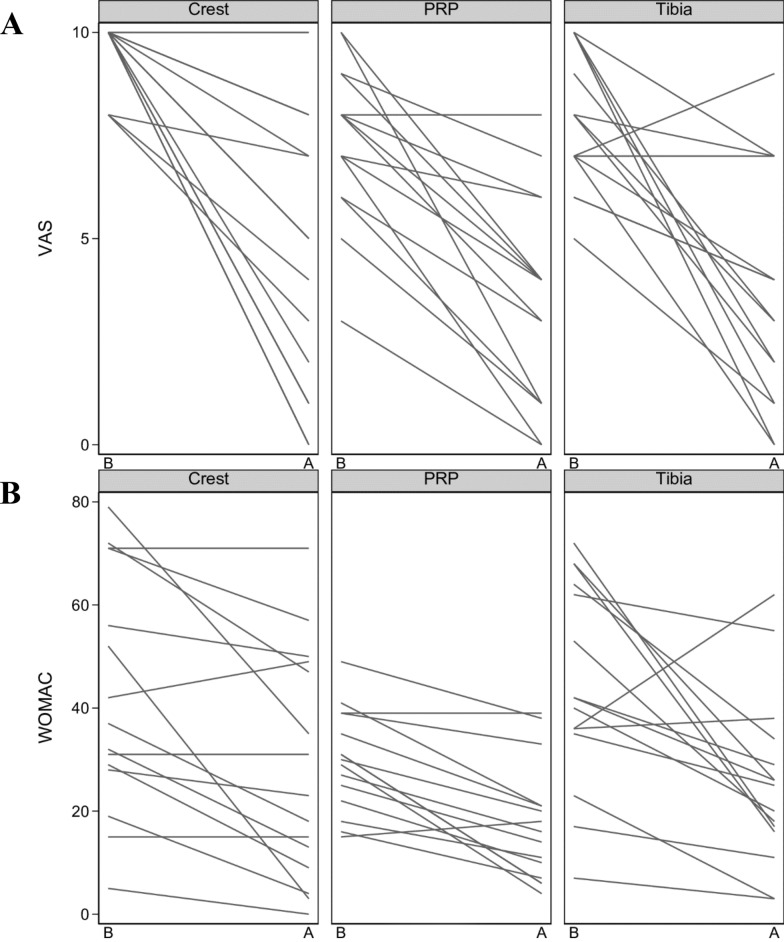
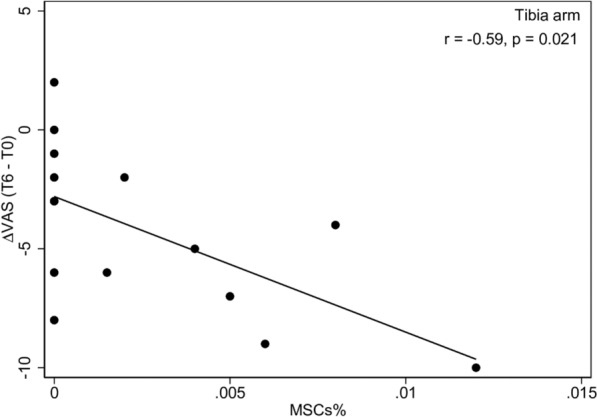
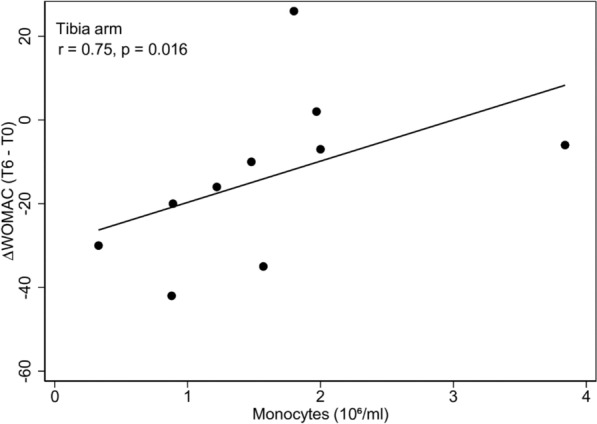
Results: Data from an intermediate analysis of 6-months follow-up, involving 15 patients in each arm, showed that the posterior iliac crest was significantly more densely populated with mononuclear cells, than the proximal tibia (p = 0.005). Flow cytometric analysis on ex vivo BMA showed a significantly greater number of MSCs in the BM-derived from the posterior iliac crest when compared with the proximal tibia (p < 0.001), together with a significantly higher number of platelets (PLTs) (p < 0.001). Surprisingly, despite these differences in cells number, the improvement in early pain and function scores, after each treatment, were statistically significant within each of the three arms. BM from the proximal tibia showed the highest ΔWOMAC, while BM from the posterior iliac crest showed the highest ΔVAS; however, these differences were not statistically significant across the three arms (p > 0.05). A better outcome, in terms of ΔVAS, was observed in patients classified as KL I-II, when treated with BMA from crest (p < 0.001) and PRP (p = 0.004). Moreover, the effect of BMA treatment on ΔVAS depends on MSCs % only in the Tibia Arm (r = -0.59, p = 0.021), where we also found a correlation between ΔWOMAC and monocytes (r = 0.75, p = 0.016).
Conclusion: The results indicate that the iliac crest yields a higher concentration of MSCs compared to the proximal tibia, however both BM, independently of the MSCs concentration, show a beneficial clinical outcome in the treatment of knee OA. Furthermore, BMA is not superior to PRP treatment.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the local ethics committee (protocol number 263/01/DG). All subjects gave their written informed consent before procedure. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures



References
-
- Buckwalter JA, Mankin HJ. Articular cartilage: degeneration and osteoarthritis, repair, regeneration, and transplantation. Instr Course Lect. 1998;47:487–504. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
