

The CCL5/CCR5/SHP2 axis sustains Stat1 phosphorylation and activates NF-κB signaling promoting M1 macrophage polarization and exacerbating chronic prostatic inflammation
- PMID: 39633456
- PMCID: PMC11619290
- DOI: 10.1186/s12964-024-01943-w
The CCL5/CCR5/SHP2 axis sustains Stat1 phosphorylation and activates NF-κB signaling promoting M1 macrophage polarization and exacerbating chronic prostatic inflammation
Abstract
Background and objective: Chronic prostatitis (CP) is a condition markered by persistent prostate inflammation, yet the specific cytokines driving its progression remain largely undefined. This study aims to identify key cytokines involved in CP and investigate their role in driving inflammatory responses through mechanistic and therapeutic exploration.
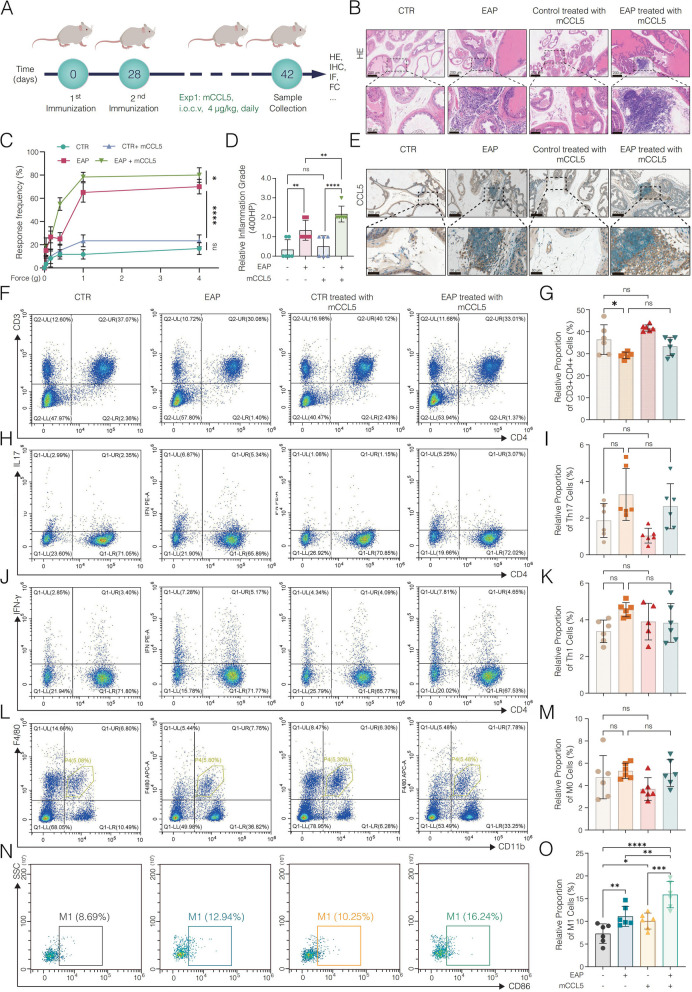
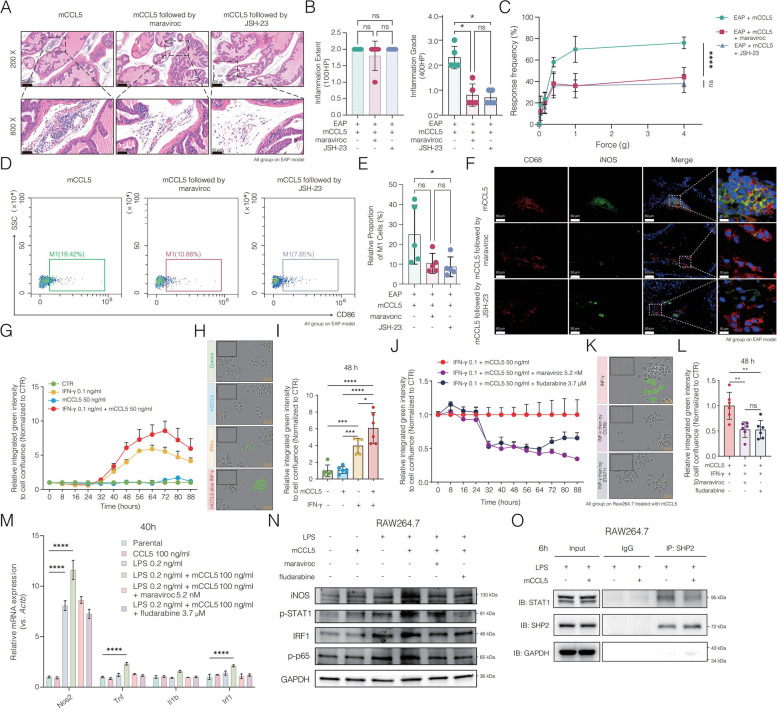
Methods: A 48-cytokine panel test was conducted to compare the plasma cytokine profiles between participants with CP-like symptoms (CP-LS) and healthy controls. Experimental autoimmune prostatitis (EAP) models were used for functional validation, with further mechanistic studies performed through in vivo and in vitro assays. Pharmacological inhibition was applied using maraviroc, and pathway inhibitors to assess therapeutic potential.
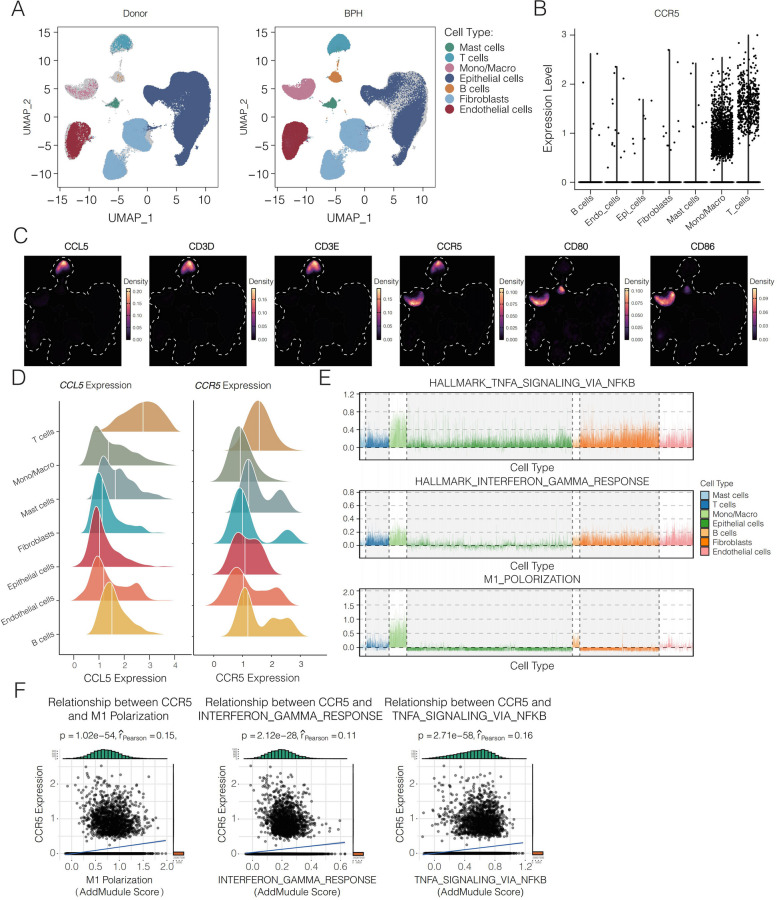
Results: Our analysis identified CCL5 as one of the most prominently elevated cytokines in CP-LS patients. Further validation in the EAP model mice confirmed elevated CCL5 levels, highlighting its role in driving prostatic inflammation. Mechanistic studies revealed that CCL5 interacts with the CCR5 receptor, promoting M1 macrophage polarization and activating key inflammatory signaling pathways, including Stat1 and NF-κB, as indicated by increased phosphorylation of Stat1 and p65. In vitro, CCL5 combined with LPS stimulation amplified these effects, further promoting M1 polarization. CCL5 also sustained Stat1 activation by inhibiting its dephosphorylation through reduced interaction with SHP2, leading to prolonged inflammatory signaling. Single-cell transcriptomics confirmed high CCR5 expression in macrophages, correlating with inflammatory pathways. Pharmacological inhibition of CCR5, or its downstream signaling, significantly reduced macrophage-driven inflammation both in vivo and in vitro.
Conclusion: These findings establish the CCL5/CCR5 axis as a critical driver of persistant prostatic inflammation and present it as a potential therapeutic target for CP.
Keywords: CCL5/CCR5 axis; Chronic prostatitis; Fludarabine; M1 macrophage; Maraviroc; NF-κB signaling; Stat1 signaling.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All procedures involving human participants, including obtaining written informed consent, were conducted in accordance with the principles outlined in the Helsinki Declaration and were approved by the Ethics Committee of the First Affiliated Hospital of Anhui Medical University on June 10, 2020 (PJ-2020–07-11). Written informed consent was obtained from all participants involved in this study. All animal experiments were conducted in compliance with the guidelines of the Animal Care and Utilization Committee of the Animal Center of Anhui Medical University, with approval (approval no. LLSC20241750). Consent for publication: Informed consent for publication was obtained from all participants involved in the study. Competing interests: The authors declare no competing interests.
Figures



References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
