

The analytical and clinical validity of AI algorithms to score TILs in TNBC: can we use different machine learning models interchangeably?
- PMID: 39634035
- PMCID: PMC11615110
- DOI: 10.1016/j.eclinm.2024.102928
The analytical and clinical validity of AI algorithms to score TILs in TNBC: can we use different machine learning models interchangeably?
Abstract
Background: Pathologist-read tumor-infiltrating lymphocytes (TILs) have showcased their predictive and prognostic potential for early and metastatic triple-negative breast cancer (TNBC) but it is still subject to variability. Artificial intelligence (AI) is a promising approach toward eliminating variability and objectively automating TILs assessment. However, demonstrating robust analytical and prognostic validity is the key challenge currently preventing their integration into clinical workflows.
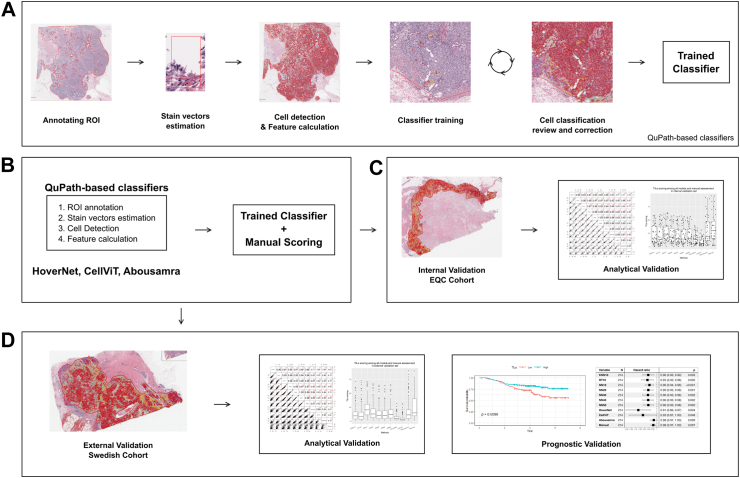
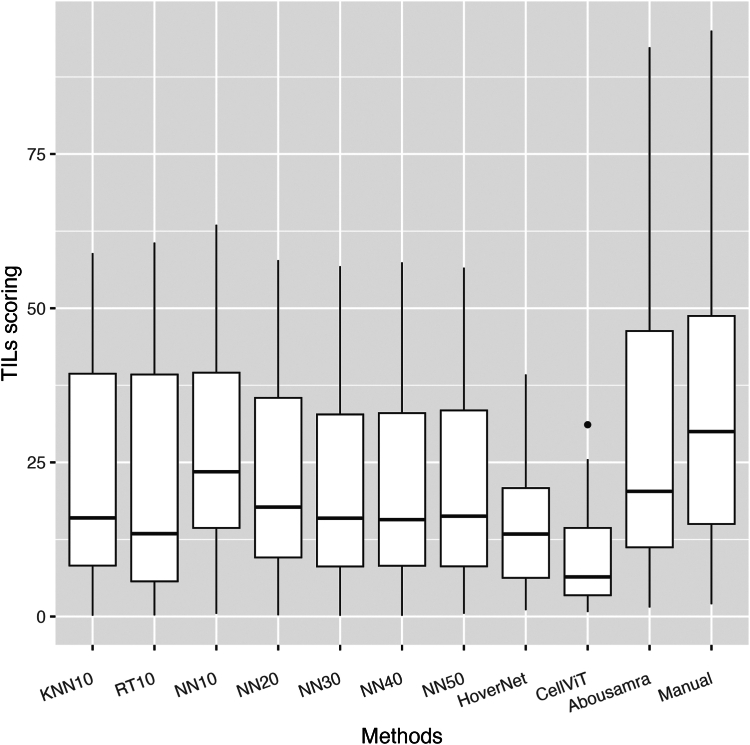
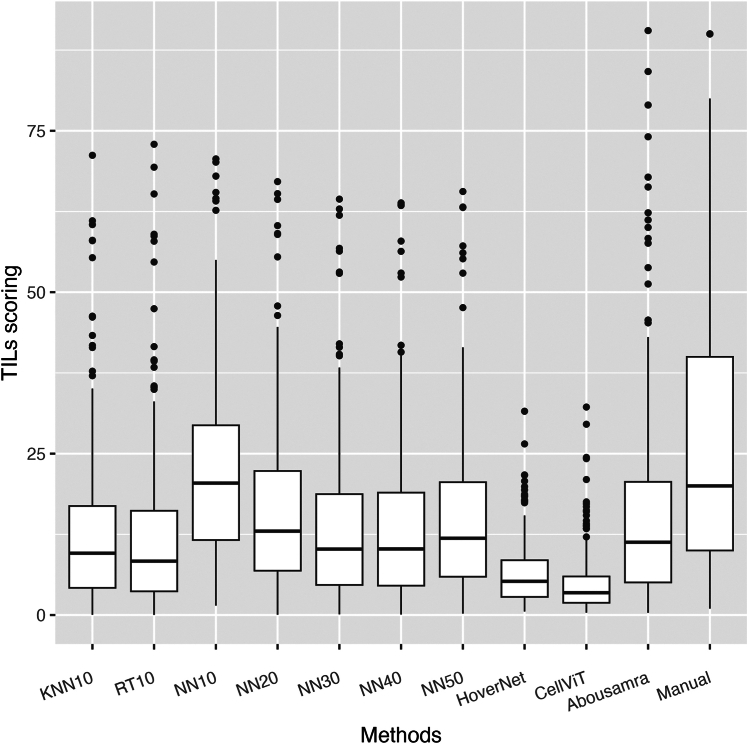
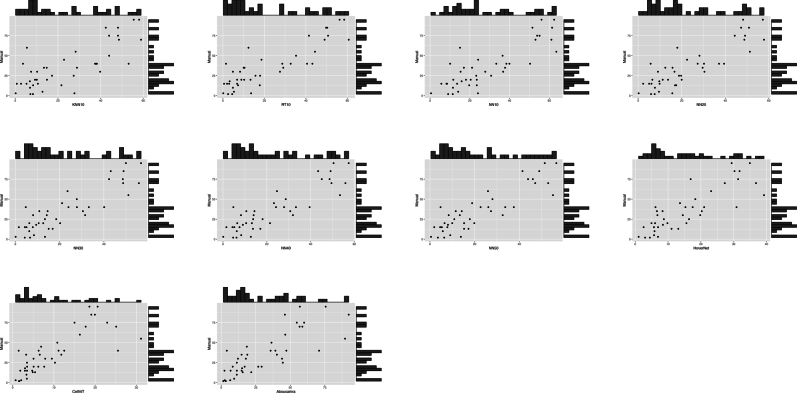
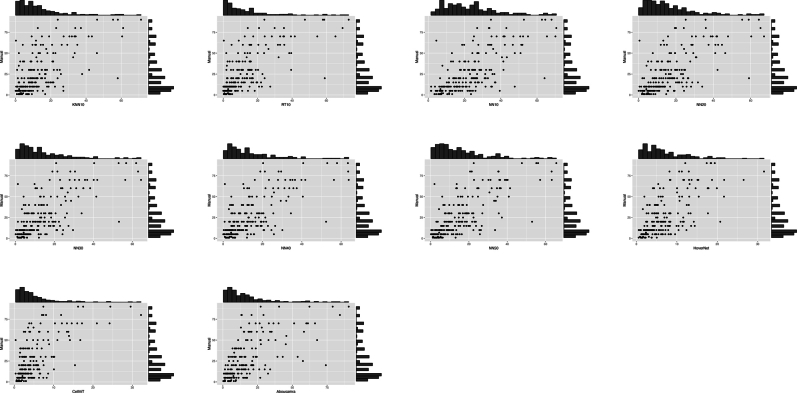
Methods: We evaluated the impact of ten AI models on TILs scoring, emphasizing their distinctions in TILs analytical and prognostic validity. Several AI-based TILs scoring models (seven developed and three previously validated AI models) were tested in a retrospective analytical cohort and in an independent prospective cohort to compare prognostic validation against invasive disease-free survival endpoint with 4 years median follow-up. The development and analytical validity set consisted of diagnostic tissue slides of 79 women with surgically resected primary invasive TNBC tumors diagnosed between 2012 and 2016 from the Yale School of Medicine. An independent set comprising of 215 TNBC patients from Sweden diagnosed between 2010 and 2015, was used for testing prognostic validity.
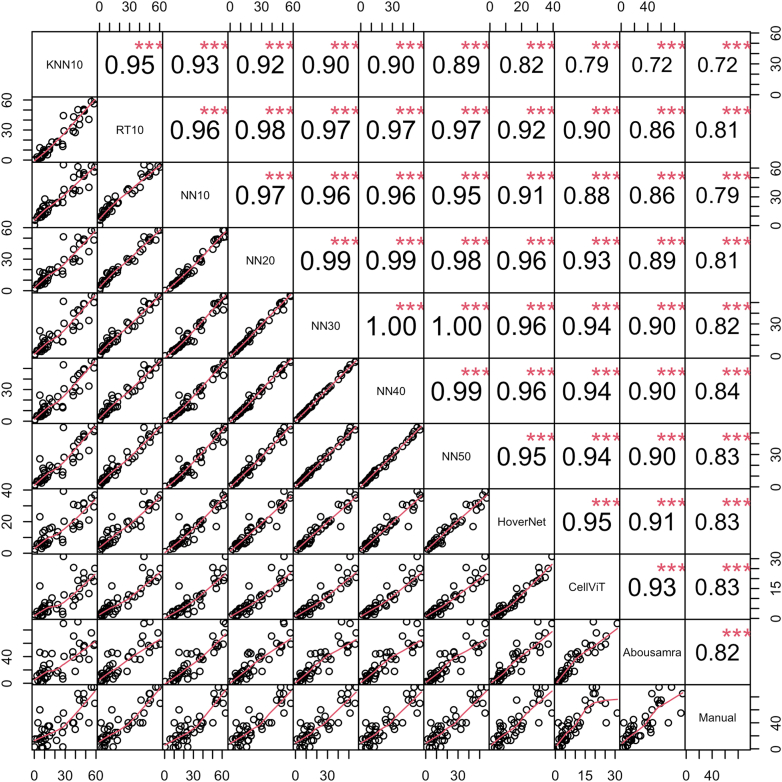
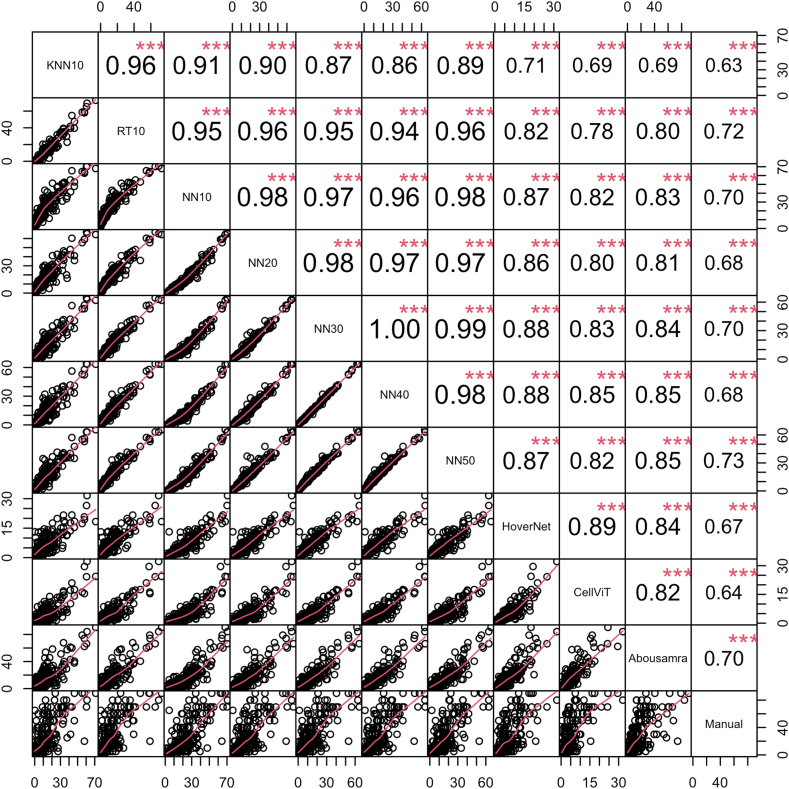
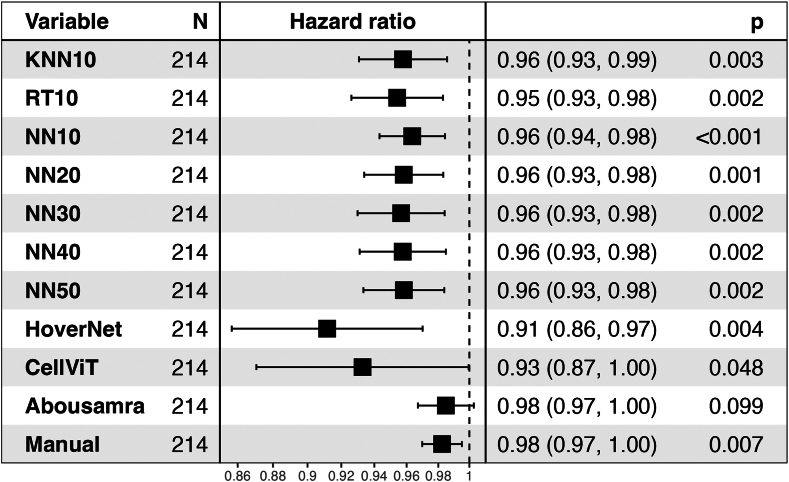
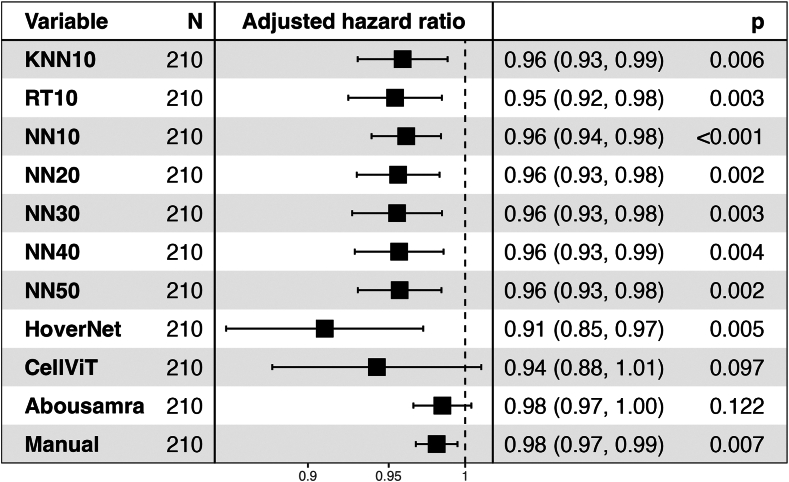
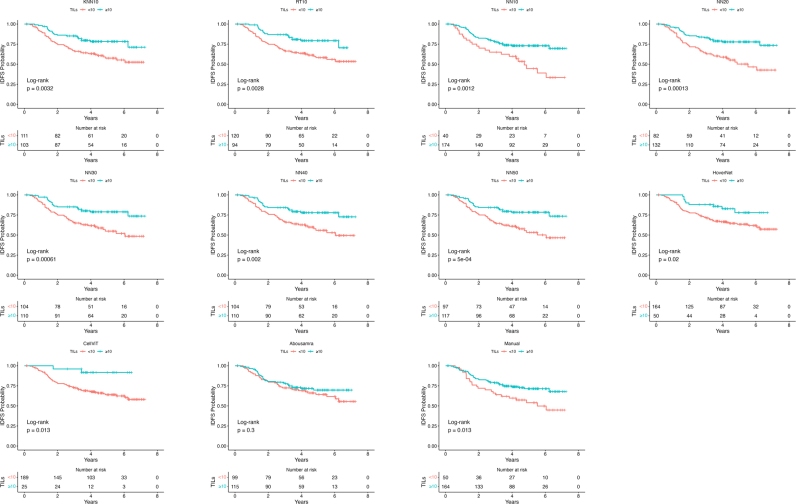
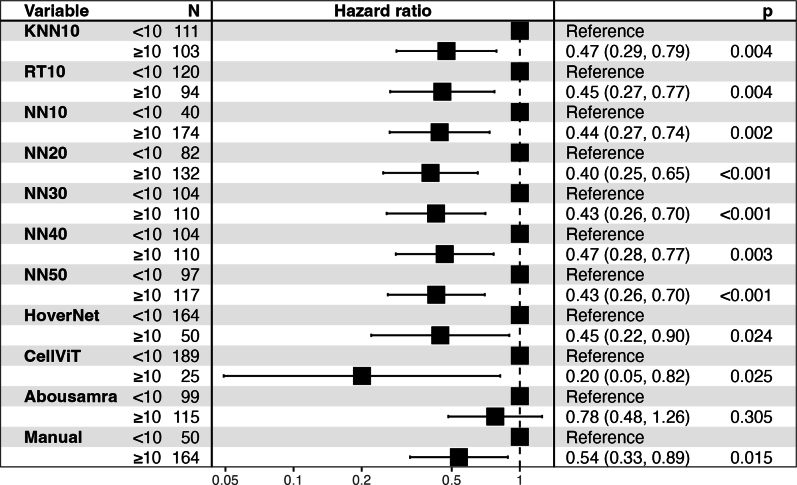
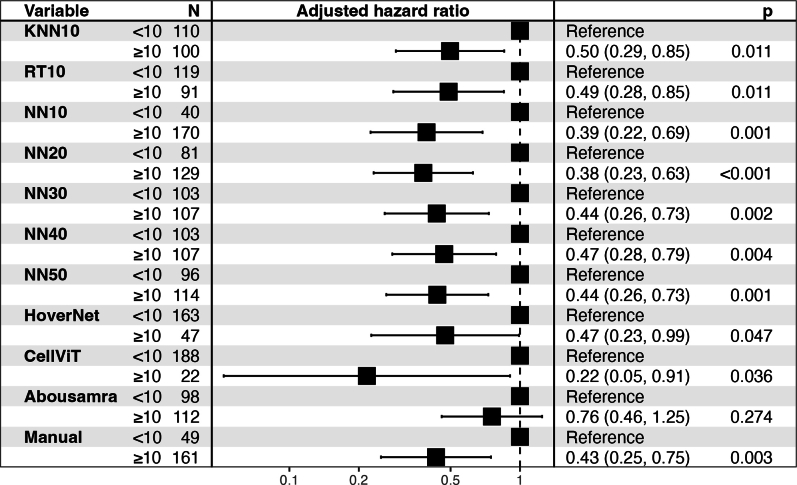
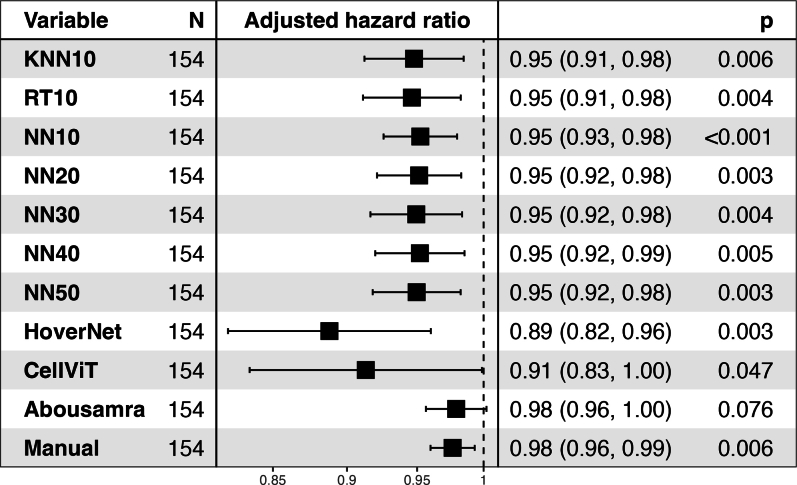
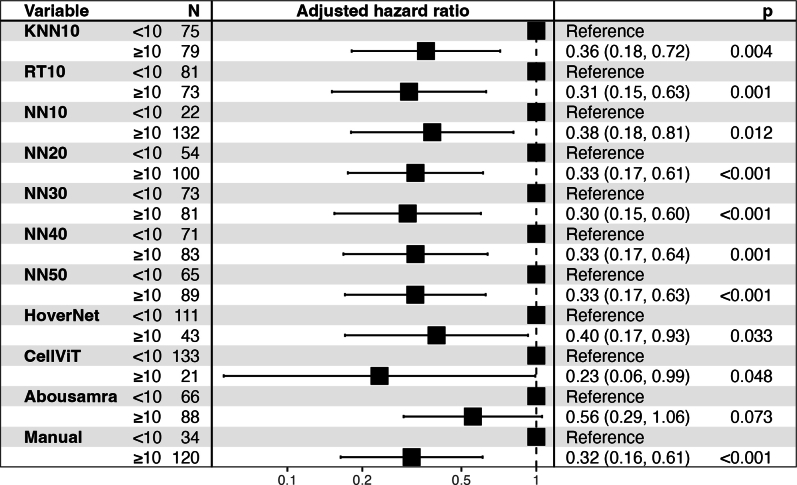
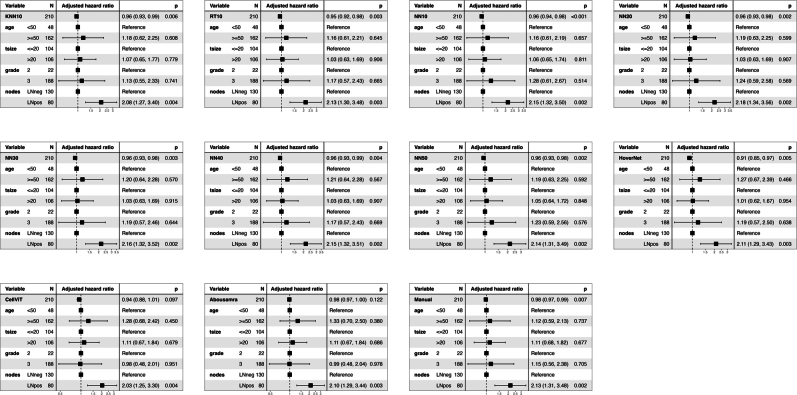
Findings: A significant difference in analytical validity (Spearman's r = 0.63-0.73, p < 0.001) is highlighted across AI methodologies and training strategies. Interestingly, the prognostic performance of digital TILs is demonstrated for eight out of ten AI models, even less extensively trained ones, with similar and overlapping hazard ratios (HR) in the external validation cohort (Cox regression analysis based on IDFS-endpoint, HR = 0.40-0.47; p < 0.004).
Interpretation: The demonstrated prognostic validity for most of the AI TIL models can be attributed to the intrinsic robustness of host anti-tumor immunity (measured by TILs) as a biomarker. However, the discrepancies between AI models should not be overlooked; rather, we believe that there is a critical need for an accessible, large, multi-centric dataset that will serve as a benchmark ensuring the comparability and reliability of different AI tools in clinical implementation.
Funding: Nikos Tsiknakis is supported by the Swedish Research Council (Grant Number 2021-03061, Theodoros Foukakis). Balazs Acs is supported by The Swedish Society for Medical Research (Svenska Sällskapet för Medicinsk Forskning) postdoctoral grant. Roberto Salgado is supported by a grant from Breast Cancer Research Foundation (BCRF).
Keywords: Artificial intelligence; Breast cancer; Deep learning; Machine learning; TILs; Tumor infiltrating lymphocytes.
© 2024 The Author(s).
Conflict of interest statement
JH has obtained speaker's honoraria or advisory board remunerations from Roche, Novartis, Pfizer, EliLilly, MSD, Gilead, Sakura and has received institutional research support from Roche, AstraZeneca, MSD and Novartis. JH is a co-founder and shareholder of Stratipath AB. AB has received honoraria from Gilead for participation in advisory board meetings and has received institutional honoraria for lectures and participation in advisory board meetings from Pfizer, Roche, Novartis and Elli Lilly. AB is a co-founder, shareholder, and CEO of SACRA Therapeutics AB. DLR has served as a Consultant/Advisor to Astra Zeneca, Cell Signaling Technology, Cepheid, Danaher, NextCure, PAIGE.AI, Regeneron, and Sanofi. Cepheid, NavigateBP, NextCure, and Leica currently fund, or have previously funded, research in his lab. RS serves on an Advisory Board and/or has a consultancy role for BMS, Roche, Owkin, Astra Zeneca, Daiichi Sankyo and Case45. RS has received research funding by Roche, Puma, Merck and BMS. RS has received travel and congress-registration support by Roche, Merck, BMS, Daiichii Sankyo and AstraZeneca. All the other authors had no potential conflicts of interest to disclose.
Figures
References
-
- Curigliano G., Burstein H.J., Gnant M., et al. Understanding breast cancer complexity to improve patient outcomes: the St Gallen international consensus conference for the primary therapy of individuals with early breast cancer 2023. Ann Oncol. 2023;34:970–986. - PubMed
-
- Denkert C., Loibl S., Noske A., et al. Tumor-associated lymphocytes as an independent predictor of response to neoadjuvant chemotherapy in breast cancer. J Clin Oncol. 2010;28(1):105–113. - PubMed
-
- Denkert C., von Minckwitz G., Darb-Esfahani S., et al. Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: a pooled analysis of 3771 patients treated with neoadjuvant therapy. Lancet Oncol. 2018;19(1):40–50. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
