

Clinical and histopathological characteristics of atrophic pigmented dermatofibrosarcoma protuberans: A retrospective study of 14 cases
- PMID: 39634408
- PMCID: PMC11616497
- DOI: 10.1016/j.heliyon.2024.e39271
Clinical and histopathological characteristics of atrophic pigmented dermatofibrosarcoma protuberans: A retrospective study of 14 cases
Abstract
Background: Dermatofibrosarcoma protuberans (DFSP) invades the dermis and subcutaneous tissue. DFSP with both atrophic and pigmentary (AP-DFSP) features is extremely rare and the clinical characteristics remain unknown. Here we aim to characterize the clinical, histopathologic and prognostic features of AP-DFSP.
Methods: Fourteen cases of patients with AP-DFSP were collected from our institution and published online, including four unreported cases and ten published cases. The clinical appearance, immunohistochemical markers, treatment, and prognosis were analyzed to obtain the clinical and histological features.
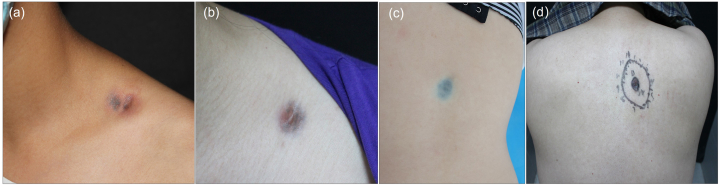
Results: There were six males and eight females with a mean age of 25 years old. The vast majority of lesions appeared in the trunk (10/14, 71.4 %) and limbs (3/14, 21.4 %), whereas a minority involved the infraorbital area (1/14, 7.2 %). The most typical manifestation was a depressed plaque-like lesion with fuchsia and bluish color. Histologically, AP-DFSP harbored both atrophic and pigmented features, presenting with a thinner dermis and intradermal melanin granules. Immunohistochemically, CD34 and vimentin were positive while S100 was negative in tumor tissues. The Ki67 index was less than 10 %. Thirteen of fourteen patients had complete excision surgery and follow-ups showed no local recurrence or distant metastasis.
Conclusion: Compared to DFSP, AP-DFSP shows more benign clinical and histological features with a good prognosis. Surgical intervention leads to a significant reduction in tumor burden and dramatically increases the likelihood of complete remission.
Keywords: Atrophic pigmented dermatofibrosarcoma protuberans; Good prognosis; Indolent character.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures



References
-
- Suzuki D., Kobayashi R., Yasuda K., Yamamoto H., Morioka K., Mikawa M., Kobayashi K. Congenital dermatofibrosarcoma protuberans in a newborn infant with a massive back tumor: favorable effects of oral imatinib on the control of residual tumor growth. J. Pediatr. Hematol. Oncol. 2011;33:e304–e306. doi: 10.1097/MPH.0b013e31822d4d21. - DOI - PubMed
LinkOut - more resources
Full Text Sources
