

The Imaging Database for Epilepsy And Surgery (IDEAS)
- PMID: 39636622
- PMCID: PMC11827737
- DOI: 10.1111/epi.18192
The Imaging Database for Epilepsy And Surgery (IDEAS)
Abstract
Objective: Magnetic resonance imaging (MRI) is a crucial tool for identifying brain abnormalities in a wide range of neurological disorders. In focal epilepsy, MRI is used to identify structural cerebral abnormalities. For covert lesions, machine learning and artificial intelligence (AI) algorithms may improve lesion detection if abnormalities are not evident on visual inspection. The success of this approach depends on the volume and quality of training data.
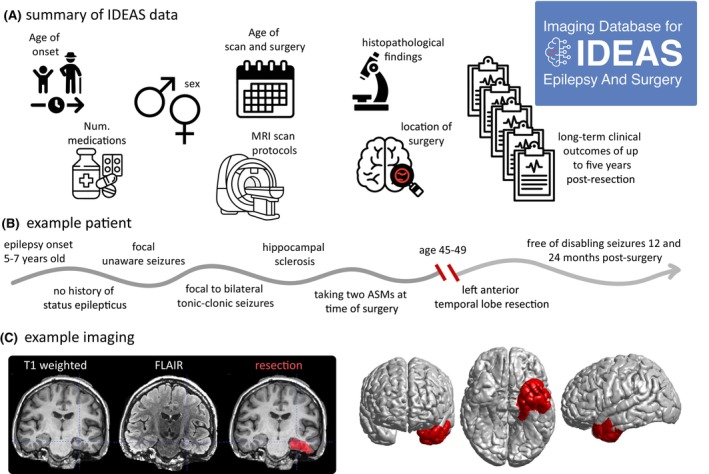
Methods: Herein, we release an open-source data set of pre-processed MRI scans from 442 individuals with drug-refractory focal epilepsy who had neurosurgical resections and detailed demographic information. We also share scans from 100 healthy controls acquired on the same scanners. The MRI scan data include the preoperative three-dimensional (3D) T1 and, where available, 3D fluid-attenuated inversion recovery (FLAIR), as well as a manually inspected complete surface reconstruction and volumetric parcellations. Demographic information includes age, sex, age a onset of epilepsy, location of surgery, histopathology of resected specimen, occurrence and frequency of focal seizures with and without impairment of awareness, focal to bilateral tonic-clonic seizures, number of anti-seizure medications (ASMs) at time of surgery, and a total of 1764 patient years of post-surgical followup. Crucially, we also include resection masks delineated from post-surgical imaging.
Results: To demonstrate the veracity of our data, we successfully replicated previous studies showing long-term outcomes of seizure freedom in the range of ~50%. Our imaging data replicate findings of group-level atrophy in patients compared to controls. Resection locations in the cohort were predominantly in the temporal and frontal lobes.
Significance: We envisage that our data set, shared openly with the community, will catalyze the development and application of computational methods in clinical neurology.
Keywords: MRI; data; epilepsy; prediction; surgery.
© 2024 The Author(s). Epilepsia published by Wiley Periodicals LLC on behalf of International League Against Epilepsy.
Conflict of interest statement
The authors have no conflict of interest to disclose.
Figures



References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
