

Pancreatic Adenocarcinoma: Long-Term Outcomes of Adjuvant Therapy in the ESPAC4 Phase III Trial
- PMID: 39637340
- PMCID: PMC11949205
- DOI: 10.1200/JCO.24.01118
Pancreatic Adenocarcinoma: Long-Term Outcomes of Adjuvant Therapy in the ESPAC4 Phase III Trial
Abstract
Purpose: The ESPAC4 trial showed that adjuvant chemotherapy with gemcitabine plus capecitabine (GemCap) produced longer overall survival (OS) than gemcitabine monotherapy. Subsequently, the PRODIGE24-CCTG PA.6 trial showed even longer survival for modified fluorouracil, folinic acid, irinotecan, and oxaliplatin (mFOLFIRINOX) than gemcitabine but had more restrictive eligibility criteria. Our aim was to analyze the ESPAC4 survival on long-term follow-up.
Methods: The OS of 732 ESPAC4 patients comparing 367 randomly assigned to gemcitabine and 365 to GemCap was previously reported after a median follow-up time of 43.2 months (95% CI, 39.7 to 45.5) and 458 deaths. Analysis was now carried out after a median follow-up of 104 months (101-108) and 566 deaths.
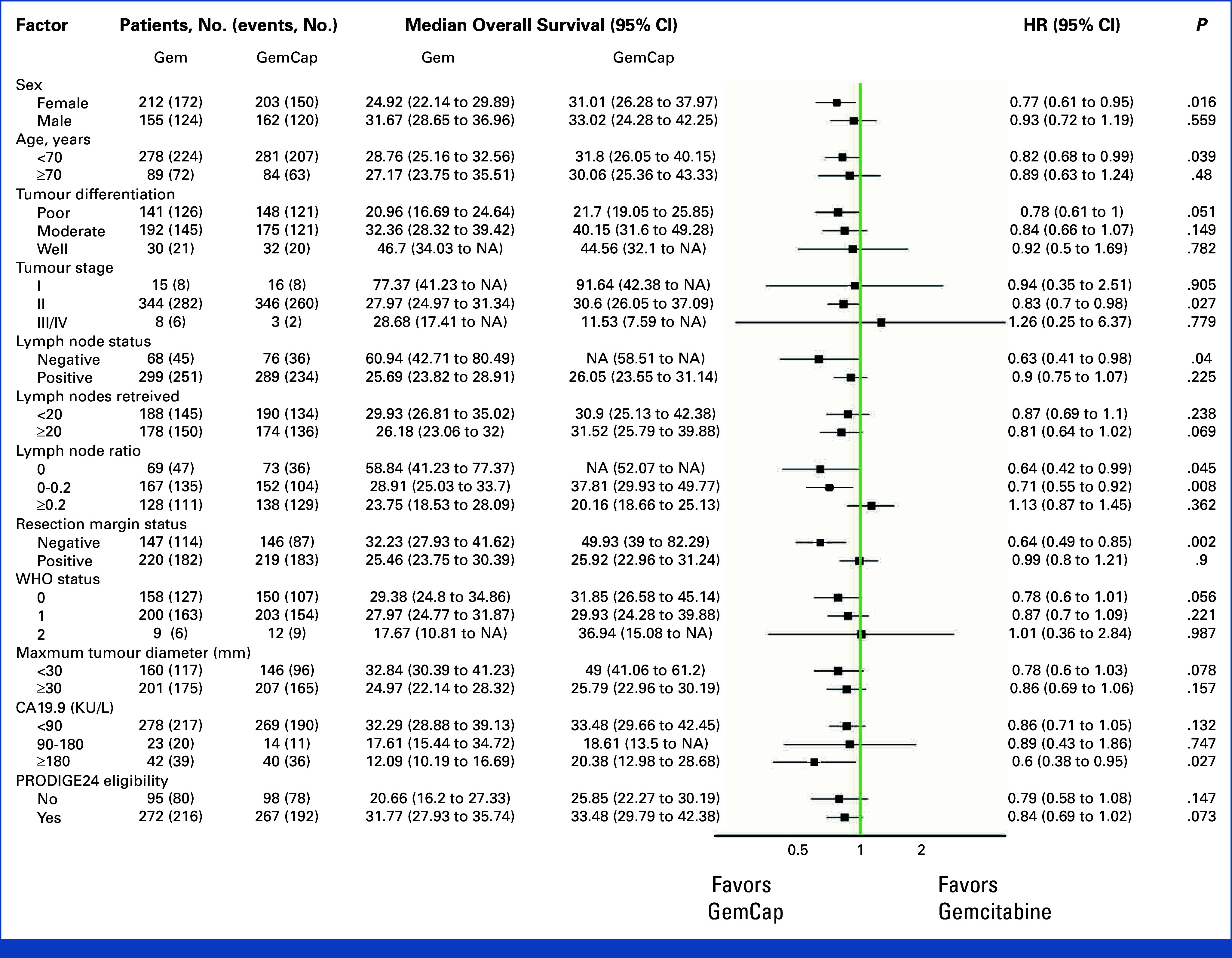
Results: The median OS was 29.5 months (27.5-32.1) for all patients, 28.4 months (25.2-32.0) in the gemcitabine group and 31.6 months (26.5-38.0) in the GemCap group (hazard ratio [HR], 0.83 [0.71 to 0.98]; P = .031). R0 patients given gemcitabine had a median survival of 32.2 months (27.9-41.6) compared with 49.9 months (39.0-82.3) for those given GemCap (HR, 0.63 [0.47 to 0.84]; P = .002). Lymph node-negative patients had significantly higher 5 year OS rates on GemCap (59% [49%-71%]) than gemcitabine (53% [42%-66%]; HR, 0.63 [0.41 to 0.98]; P = .04) but not those with positive lymph nodes (P = .225). The OS advantage for GemCap was retained in the PRODIGE24 subgroup of 193 (26.4%) ESPAC4 patients not eligible for PRODIGE24 with a median survival of 20.7 (16.2-27.3) months in patients allocated to gemcitabine compared with 25.9 (22.3-30.2) months for ineligible patients allocated to GemCap (HR, 0.71 [95% CI, 0.52 to 0.98]; χ2log-rank-1df = 4.31; P = .038).
Conclusion: GemCap is a standard option for patients not eligible for mFOLFIRINOX. Exploratory evidence suggests that GemCap may be particularly efficacious in R0 patients and also in lymph node-negative patients.
Trial registration: ClinicalTrials.gov ISRCTN96397434.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures



References
-
- Strobel O, Neoptolemos J, Jäger D, et al. : Optimizing the outcomes of pancreatic cancer surgery. Nat Rev Clin Oncol 16:11-26, 2019 - PubMed
-
- Springfeld C, Ferrone CR, Katz MHG, et al. : Neoadjuvant therapy for pancreatic cancer. Nat Rev Clin Oncol 20:318-337, 2023 - PubMed
-
- Siegel RL, Giaquinto AN, Jemal A: Cancer statistics, 2024. CA Cancer J Clin 74:12-49, 2024 - PubMed
-
- Neoptolemos JP, Dunn JA, Stocken DD, et al. : Adjuvant chemoradiotherapy and chemotherapy in resectable pancreatic cancer: A randomised controlled trial. Lancet 358:1576-1585, 2001 - PubMed
-
- Neoptolemos JP, Stocken DD, Friess H, et al. : A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med 350:1200-1210, 2004 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
