

Characterizing the genetic architecture of drug response using gene-context interaction methods
- PMID: 39637863
- PMCID: PMC11701255
- DOI: 10.1016/j.xgen.2024.100722
Characterizing the genetic architecture of drug response using gene-context interaction methods
Abstract
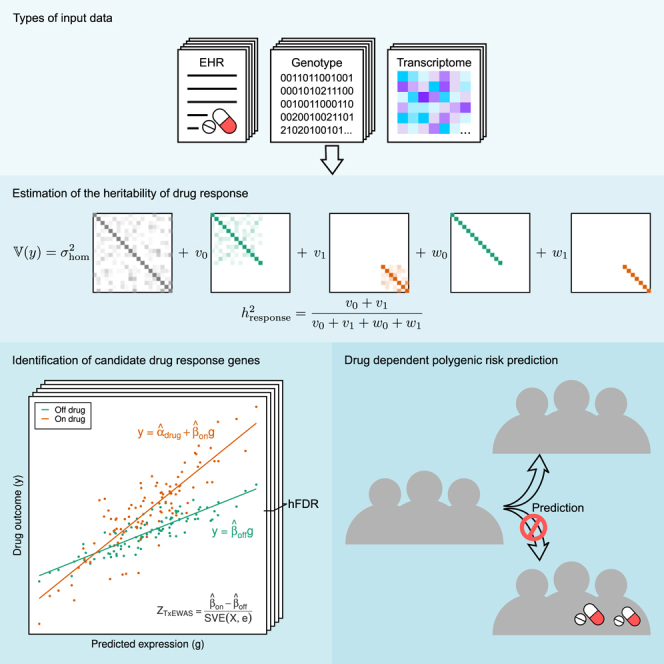
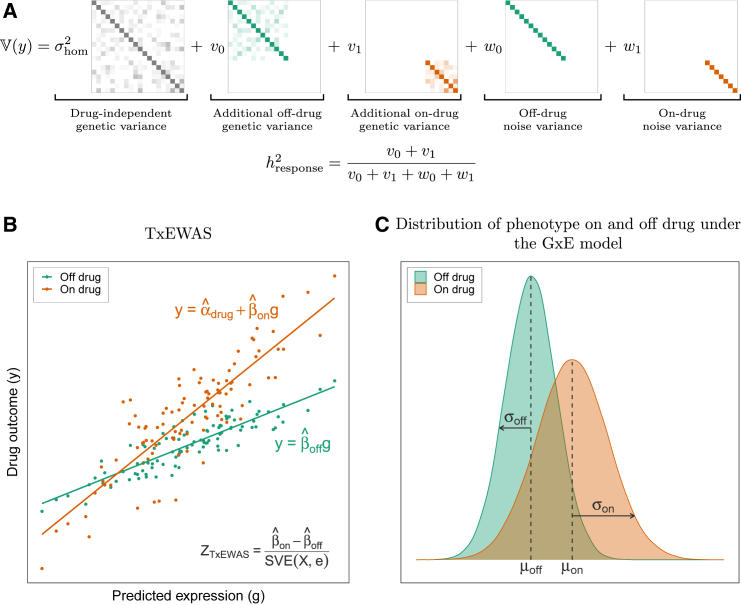
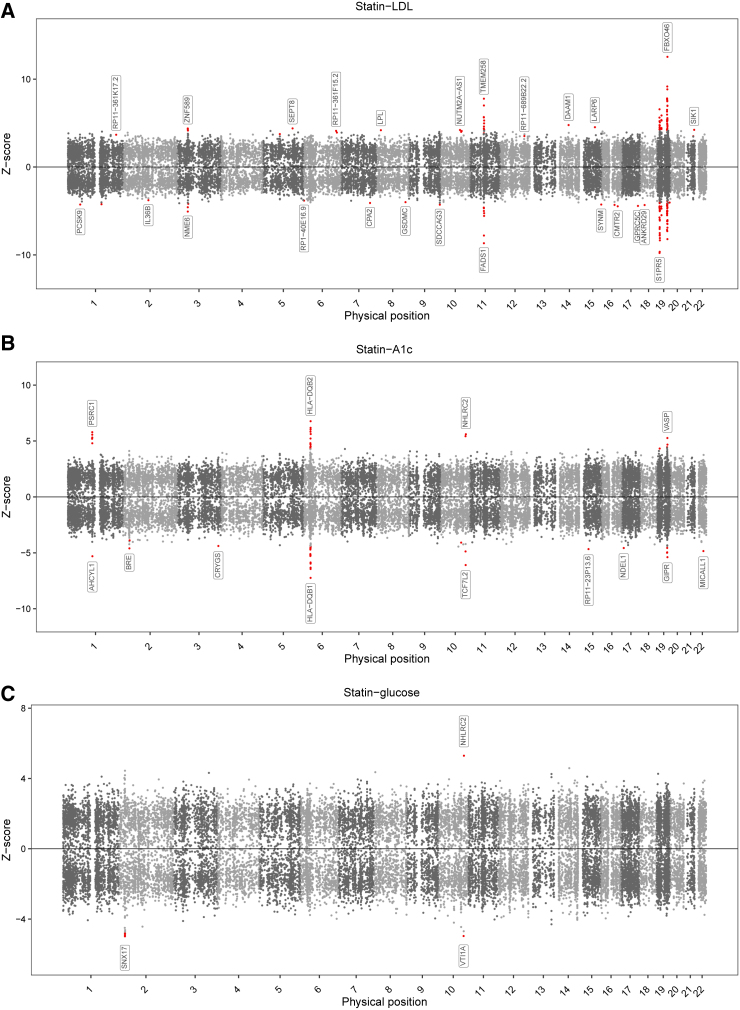
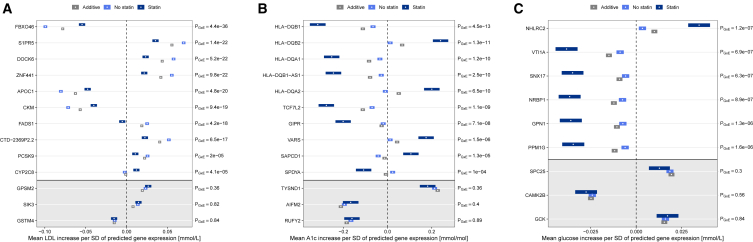
Identifying factors that affect treatment response is a central objective of clinical research, yet the role of common genetic variation remains largely unknown. Here, we develop a framework to study the genetic architecture of response to commonly prescribed drugs in large biobanks. We quantify treatment response heritability for statins, metformin, warfarin, and methotrexate in the UK Biobank. We find that genetic variation modifies the primary effect of statins on LDL cholesterol (9% heritable) as well as their side effects on hemoglobin A1c and blood glucose (10% and 11% heritable, respectively). We identify dozens of genes that modify drug response, which we replicate in a retrospective pharmacogenomic study. Finally, we find that polygenic score (PGS) accuracy varies up to 2-fold depending on treatment status, showing that standard PGSs are likely to underperform in clinical contexts.
Keywords: gene-environment interactions; genetic heterogeneity; genetic testing; heritability; heteroskedasticity; personalized medicine; pharmacogenomics.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures
References
-
- Mega J.L., Simon T., Collet J.-P., Anderson J.L., Antman E.M., Bliden K., Cannon C.P., Danchin N., Giusti B., Gurbel P., et al. Reduced-Function CYP2C19 Genotype and Risk of Adverse Clinical Outcomes Among Patients Treated With Clopidogrel Predominantly for PCI: A Meta-analysis. JAMA. 2010;304:1821–1830. doi: 10.1001/jama.2010.1543. - DOI - PMC - PubMed
