

Monitoring individualized glucose levels predicts risk for bradycardia in type 2 diabetes patients with chronic kidney disease: a pilot study
- PMID: 39638855
- PMCID: PMC11621348
- DOI: 10.1038/s41598-024-81983-x
Monitoring individualized glucose levels predicts risk for bradycardia in type 2 diabetes patients with chronic kidney disease: a pilot study
Abstract
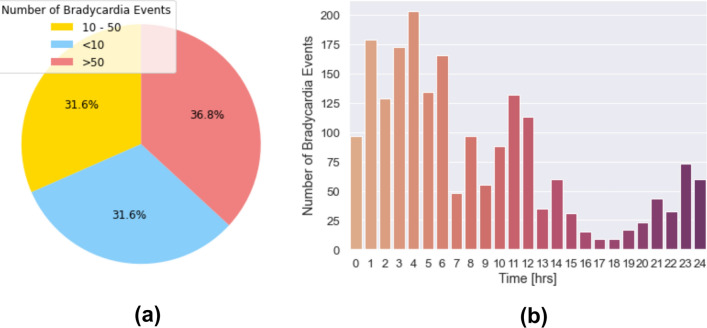
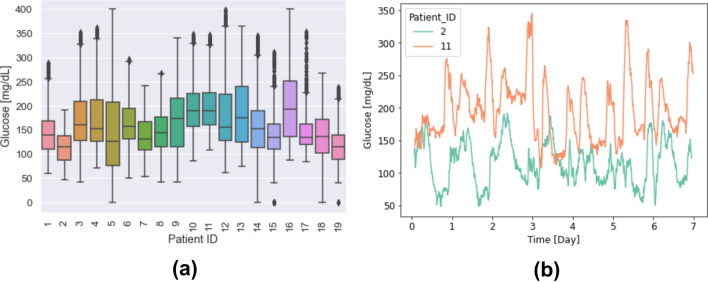
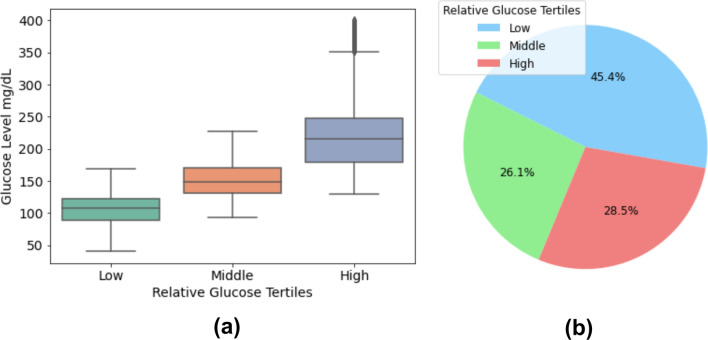
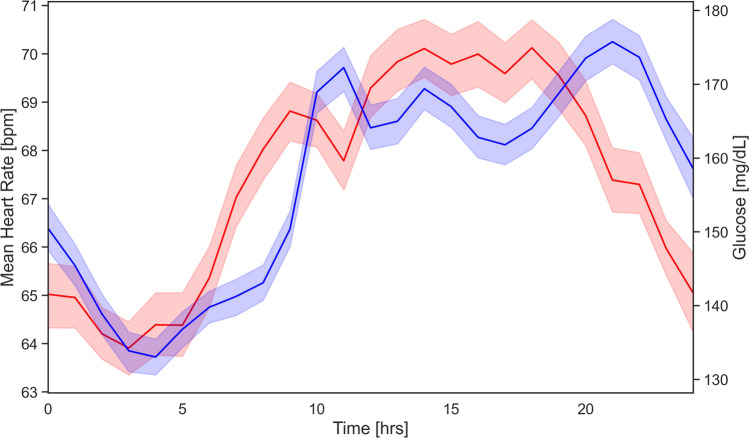
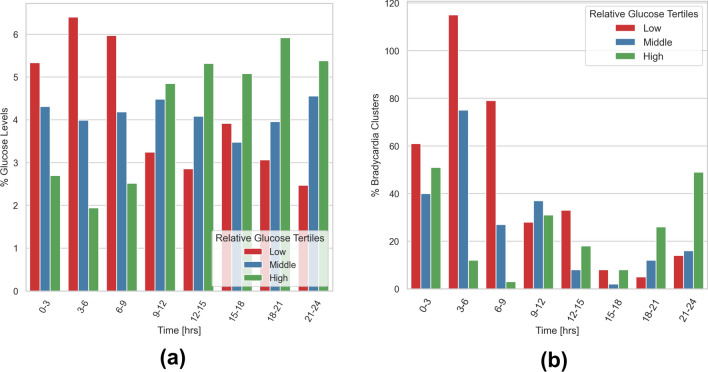
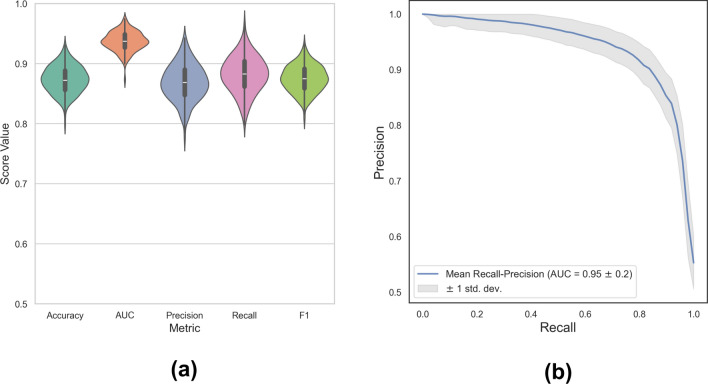
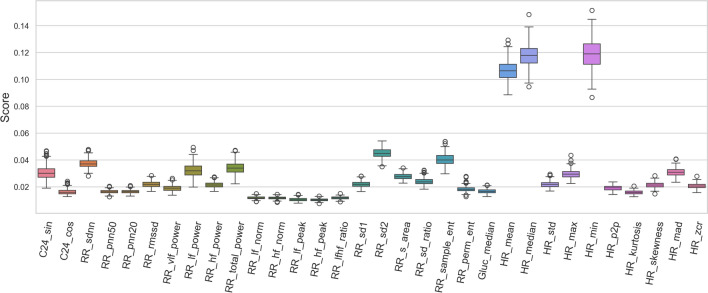
Patients with diabetes mellitus (DM) and chronic kidney disease (CKD) exhibit an elevated risk for cardiac arrhythmias, such as bradycardia, which may potentially lead to sudden cardiac death (SCD). While hypoglycemia, defined as a critical drop in glucose levels below the normal range, has long been associated with adverse cardiovascular events, recent studies have highlighted the need for a comprehensive reevaluation of its direct impact on cardiovascular outcomes, particularly in high-risk populations such as those with DM and CKD. In this study, we investigated the association between glucose levels and bradycardia by simultaneously monitoring interstitial glucose (IG) and ECG for 7 days in insulin-treated patients with DM and CKD. We identified bradycardia episodes in 19 of 85 patients (22%) and associated these episodes with personalized low, medium, and high relative glucose levels. Our analysis revealed a significant increase in bradycardia frequency during periods of lowest relative glucose, particularly between 06:00-09:00 and 12:00-15:00. Furthermore, leveraging a Random Forests classifier, we achieved a promising area under the curve (AUC) of 0.94 for predicting bradyarrhythmias using glucose levels and heart rate variability features. Contrary to previous findings, only 4% of bradycardia episodes in our study population occurred at glucose levels of 70 mg/dL or lower, with 28% observed at levels exceeding 180 mg/dL. Our findings not only highlight the strong correlation between relative glucose levels, heart rate parameters, and bradycardia onset but also emphasize the need for a more personalized definition of hypoglycemia to understand its relationship with bradyarrhythmias in high-risk DM and CKD patient populations.
Keywords: Bradycardia; Chronic kidney disease; Diabetes mellitus; Glucose monitoring; Hypoglycemia; Machine learning; Personalized medicine.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
References
-
- Carrero, J. J. et al. Sex differences in the impact of diabetes on mortality in chronic dialysis patients. Nephrology Dialysis Transplantation26, 270–276 (2011). - PubMed
-
- Bergner, D. W. & Goldberger, J. J. Diabetes mellitus and sudden cardiac death: what are the data?. Cardiology journal17, 117–129 (2010). - PubMed
-
- Myerburg, R. J. & Junttila, M. J. Sudden cardiac death caused by coronary heart disease. Circulation125, 1043–1052 (2012). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
