

Metabolic imaging distinguishes ovarian cancer subtypes and detects their early and variable responses to treatment
- PMID: 39639170
- PMCID: PMC11850285
- DOI: 10.1038/s41388-024-03231-w
Metabolic imaging distinguishes ovarian cancer subtypes and detects their early and variable responses to treatment
Abstract
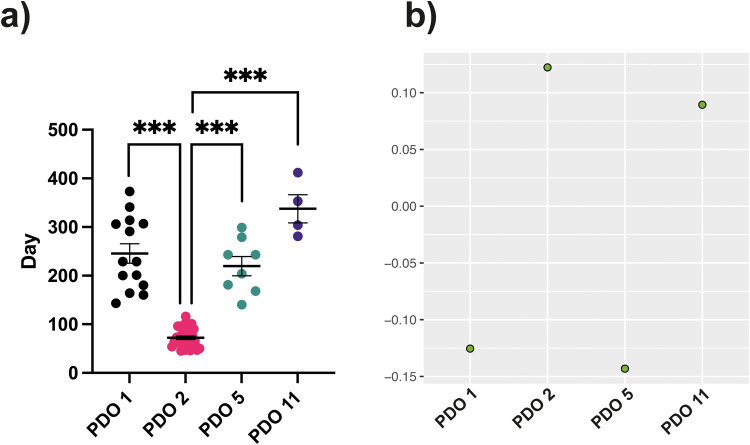
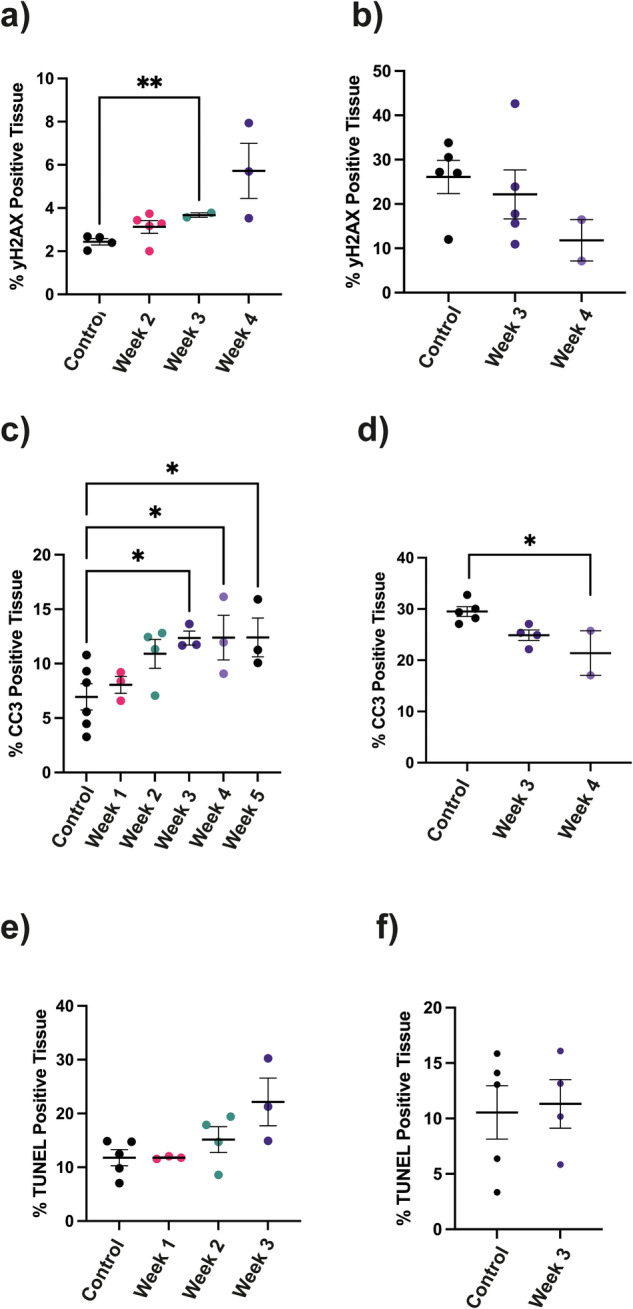
High grade serous ovarian cancer displays two metabolic subtypes; a high OXPHOS subtype that shows increased expression of genes encoding electron transport chain components, increased oxygen consumption, and increased chemosensitivity, and a low OXPHOS subtype that exhibits glycolytic metabolism and is more drug resistant. We show here in patient-derived organoids and in the xenografts obtained by their subcutaneous implantation that the low OXPHOS subtype shows higher lactate dehydrogenase activity and monocarboxylate transporter 4 expression than the high OXPHOS subtype and increased lactate labeling in 13C magnetic resonance spectroscopy (MRS) measurements of hyperpolarized [1-13C]pyruvate metabolism. There was no difference between the subtypes in PET measurements of 2-deoxy-2-[fluorine-18]fluoro-D-glucose ([18F]FDG) uptake. Both metabolic imaging techniques could detect the early response to Carboplatin treatment in drug-sensitive high OXPHOS xenografts and no response in drug-resistant in low OXPHOS xenografts. 13C magnetic resonance spectroscopic imaging of hyperpolarized [1-13C]pyruvate metabolism has the potential to be used clinically to distinguish low OXPHOS and high OXPHOS tumor deposits in HGSOC patients and to detect their differential responses to treatment.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests. Ethics approval and consent to participate: All methods were performed in accordance with the relevant guidelines and regulations. Organoids were derived from tumor samples collected on the prospective cohort study Cambridge Translational Cancer Research Ovarian Study 04 (CTCR-OV04), with IRAS project ID 4853, and which was approved by the Institutional Ethics Committee (REC reference number 08 /H0306/61). Patients provided written, informed consent for participation and for the use of their donated tissue for laboratory studies.
Figures






References
-
- Ferlay J, Colombet M, Soerjomataram I, Dyba T, Randi G, Bettio M, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries and 25 major cancers in 2018. Eur J Cancer. 2018;103:356–87. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
