

The effects of blood cell salvage on transfusion requirements after decannulation from veno-venous extracorporeal membrane oxygenation: an emulated trial analysis
- PMID: 39639320
- PMCID: PMC11619385
- DOI: 10.1186/s13054-024-05177-7
The effects of blood cell salvage on transfusion requirements after decannulation from veno-venous extracorporeal membrane oxygenation: an emulated trial analysis
Abstract
Background: Veno-venous extracorporeal membrane oxygenation (VV-ECMO) is a supportive therapy for acute respiratory failure with increased risk of packed red blood cells (PRBC) transfusion. Blood cell salvage (BCS) aims to reduce blood transfusion, but its efficacy is unclear. This study aimed to estimate the effect of BCS at the time of removal of the ECMO circuit (ECMO decannulation) on PRBC transfused.
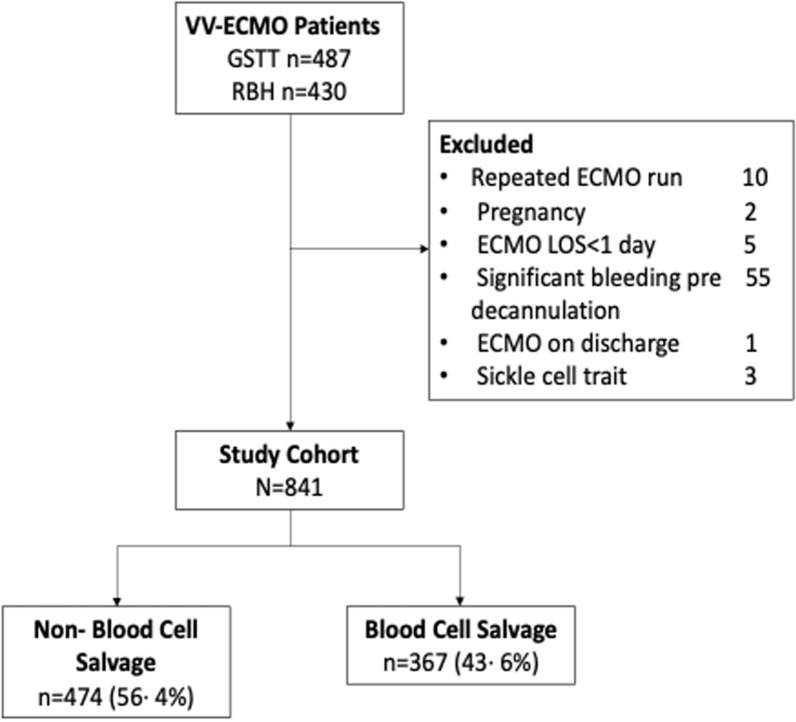
Methods: To compare BCS to non-blood cell salvage (n-BCS), we conducted an emulated trial of patients at two ECMO centres in the United Kingdom. We used inverse propensity of treatment weighting to control for confounding and estimated the average treatment effect of BCS on PRBC transfused within two days of decannulation, and on changes in haemoglobin (Hb).
Results: We included 841 patients who underwent VV-ECMO decannulation. The estimated marginal mean number of PRBC transfused when using BCS was 0·2 (95%CI: 0·16, 0·25) units compared to 0·51 (95%CI: 0·44, 0·59) units with n-BCS; an average treatment effect of -0·31 (95%CI: -0·40, -0·22) units. BCS reduced the risk of receiving any PRBC transfusion by 17·1% (95%CI: 11·1%, 22·9%) equating to a number needed to treat for any PRBC transfusion of 6 (95%CI: 5, 9). The difference in expected Hb levels after decannulation between BCS and n-BCS was 5·0 (95%CI: 4·2, 5·8) g/L.
Conclusions: The use of BCS during VV-ECMO decannulation may be an effective strategy to augment haemoglobin levels and reduce PRBC transfusions.
Keywords: ARDS; Blood cell salvage; PRBC; Transfusion; VV ECMO.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: RHK received funding from UK Research and Innovation through the Future Leaders Fellowship (MR/S017968/1, MR/X015017/1), with payments made to the London School of Hygiene & Tropical Medicine (LSHTM). BVP participated in the Data Safety Monitoring Board for Novartis and received speaker fees from Medtronic. LR received funding from NIHR and ICS, speaker fees from Dräger Medical, and participated in the Data Safety Monitoring Board for Hamilton Medical. AR is the Chief Medical Officer at Volition Diagnostics Limited, a diagnostic start-up. LG received consulting fees and speaker fees from General Electric, Kures, and Sidam, and participated in the Data Safety Monitoring Board for Grifols. DFM received grants from NIHR, Innovate UK, MRC, Novavax, Northern Ireland HSC R&D division, Randox, Wellcome Trust, and Queen’s University Belfast. He collaborates with Bayer, Aptarion, Direct Biologics, Aviceda, GlaxoSmithKline, Boehringer Ingelheim, Novartis, Eli Lilly, and SOBI. He also received speaker fees from GlaxoSmithKline and participated in the Data Safety Monitoring Board for Vir Biotechnology, Inc. and Faron Pharmaceuticals. DFM is the Co-director of Research for the Intensive Care Society, Director of the EME Programme for MRC and NIHR, and Scientific Director for NIHR Programmes. All other authors reported no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
