

Differential prevalence and prognostic value of metabolic syndrome components among patients with MASLD
- PMID: 39640221
- PMCID: PMC11617726
- DOI: 10.1016/j.jhepr.2024.101193
Differential prevalence and prognostic value of metabolic syndrome components among patients with MASLD
Abstract
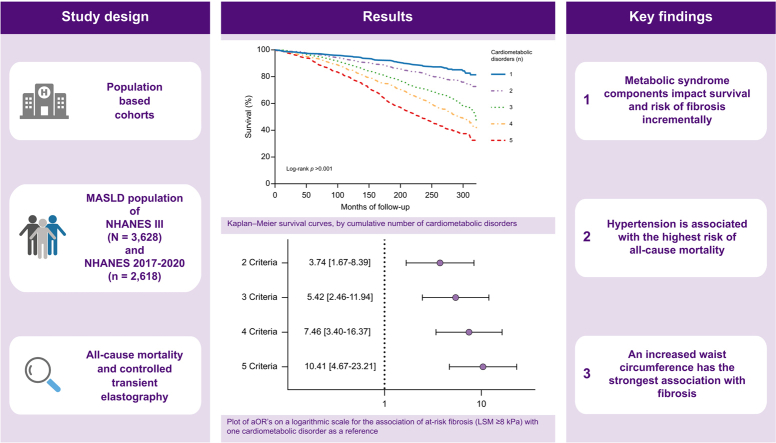
Background & aims: Metabolic dysfunction-associated steatotic liver disease (MASLD) is becoming increasingly prevalent in the general population. This study aimed at describing the cardiometabolic burden of the MASLD population and to identify patients at the highest risk of all-cause mortality and liver fibrosis.
Methods: We analysed individuals with MASLD enrolled in the National Health and Nutrition Survey (NHANES) III study (N = 3,628) and in the NHANES 2017-2020 study (n = 2,618). MASLD was defined as hepatic steatosis (by ultrasonography or controlled attenuation parameter), together with cardiometabolic dysfunction. Primary endpoints were all-cause mortality and liver fibrosis (liver stiffness measurement ≥8 kPa). Regression models were adjusted for age, sex, race, marital status, education, and smoking, and results were stratified by age groups (20-40, 40-60, 60-80 years).
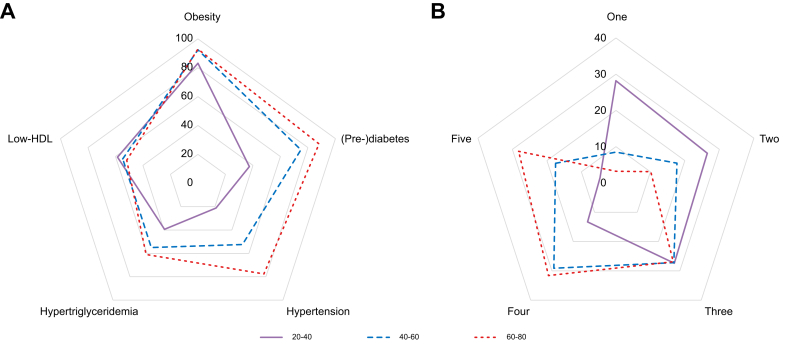
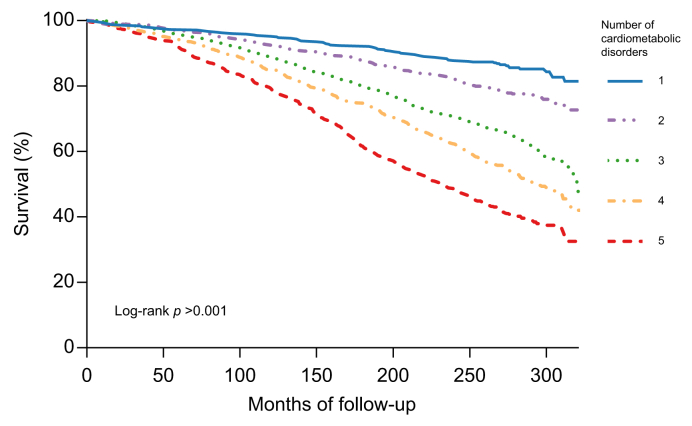
Results: Among the total MASLD population (median age = 48, [25th to 75th percentiles: 36-62] years, 44.8% males), 65% had three or more cardiometabolic disorders. The most frequent were obesity (89.1%), (pre-) diabetes (66.6%), and low-HDL (54.7%). During a median follow-up of 22.3 (25th to 75th percentiles: 16.9-24.2) years, 1,405 deaths occurred. Hypertension (adjusted hazard ratio [aHR] 1.42, 95% CI 1.26-1.61), (pre-)diabetes (aHR 1.28, 95% CI 1.09-1.49), and hypertriglyceridaemia (aHR 1.19, 95% CI 1.05-1.34) were the strongest predictors of all-cause mortality. Consistent results were obtained regarding the association between cardiometabolic disorders and fibrosis. Here, increased waist circumference (adjusted odds ratio [aOR] 3.45, 95% CI 1.44-8.25), (pre-)diabetes (aOR 1.90, 95% CI 1.44-2.25), and hypertension (aHR 1.84, 95% CI 1.40-2.43) showed the strongest associations.
Conclusions: MASLD patients vary greatly in their cardiometabolic burden and consequently, in their prognosis. Our results highlight MASLD as a disease spectrum rather than as a single disease entity, necessitating an individualised treatment approach.
Impact and implications: The increasing cardiometabolic burden and incidence of MASLD, especially among younger adults, stresses the importance of the current study.2 Understanding the disease burden of MASLD patients is key, but can be challenging for healthcare professionals. Results from the current study indicate that cardiometabolic risk management is particularly warranted in the younger adult population, with specific attention to hypertension and (pre-)diabetes.
Keywords: Fibrosis; Metabolic dysfunction associated fatty liver disease; Metabolic-dysfunction associated steatotic liver disease; Mortality; Non-alcoholic fatty liver disease; Steatotic liver disease.
© 2024 The Authors.
Figures

References
-
- Le M.H., Le D.M., Baez T.C., et al. Global incidence of non-alcoholic fatty liver disease: a systematic review and meta-analysis of 63 studies and 1,201,807 persons. J Hepatol. 2023;79:287–295. - PubMed
-
- Younossi Z.M., Marchesini G., Pinto-Cortez H., Petta S. Epidemiology of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis: implications for liver transplantation. Transplantation. 2019;103:22–27. - PubMed
-
- Younossi Z., Anstee Q.M., Marietti M., et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15:11–20. - PubMed
-
- Devarbhavi H., Asrani S.K., Arab J.P., et al. Global burden of liver disease: 2023 update. J Hepatol. 2023;79:516–537. - PubMed
LinkOut - more resources
Full Text Sources
