

Bow Hunter's syndrome surgical approach and outcome: Two new cases and literature review
- PMID: 39640315
- PMCID: PMC11618828
- DOI: 10.25259/SNI_633_2024
Bow Hunter's syndrome surgical approach and outcome: Two new cases and literature review
Abstract
Background: Bow Hunter's syndrome (BHS) is a rare entity known as rotational vertebral artery occlusion syndrome. Classically, it presents with nausea, vertigo, and dizziness elicited by extension or rotation of the neck. There are several management approach modalities, including surgical and nonsurgical alternatives.
Methods: We conducted an electronic database search on PubMed and Scopus. The search was performed on February 18, 2024, using a combination of keywords related to Bow Hunter Syndrome regarding management. From the latter query, 97 results followed, from which we included 76 and excluded 21 due to the information being irrelevant to our study and non-retrievable publications.
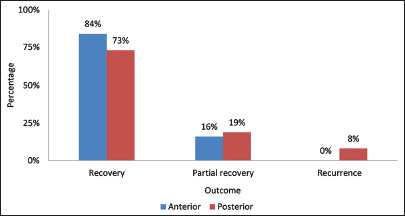
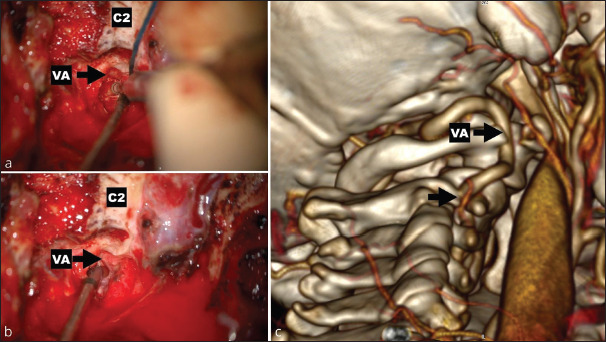
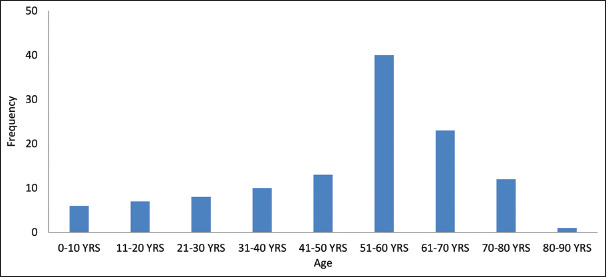
Results: A total of 121 patients were retrieved. The mean age of presentation was 50 years, with a female-to-male ratio of 3:1. There were 108 adult cases, and only 13 were pediatric and adolescents. Symptoms were elicited by right rotation (46%). The most affected levels were C1-C2 (44%). The anterior approach was the most common (40%) and had a better outcome (84%), followed by the posterior (30%), which had more cases with partial recovery (19% vs. 16%).
Conclusion: BHS management is still challenging as there are many factors that we must consider when deciding on the approach. There is inconclusive evidence on the proper management of these patients. Although the suggestions found in our review and our experience are valuable, no definitive management ensures a good quality of life and outcome for these patients. Further research is needed on this topic.
Keywords: Artery; Bow; Insufficiency; Management; Occlusion; Vertebral.
Copyright: © 2024 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Algattas H, Mitha R, Agarwal N, Lang MJ. Bow hunter syndrome: An illustrative case and operative management. World Neurosurg. 2024;182:135. - PubMed
-
- Anaizi AN, Sayah A, Berkowitz F, McGrail K. Bow Hunter’s syndrome: The use of dynamic magnetic resonance angiography and intraoperative fluorescent angiography. J Neurosurg Spine. 2014;20:71–4. - PubMed
-
- Bando K, Okazaki T, Mure H, Korai M, Takagi Y. A Juvenile case of Bow Hunter’s syndrome caused by atlantoaxial dislocation with vertebral artery dissecting aneurysm. World Neurosurg. 2020;137:393–7. - PubMed
-
- Bergl PA. Provoked dizziness from Bow Hunter’s syndrome. Am J Med. 2017;130:e375–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous