

External validation of the Leiden Thrombosis Recurrence Risk Prediction models (L-TRRiP) for the prediction of recurrence after a first venous thrombosis in the Heart and Vascular Health study
- PMID: 39640909
- PMCID: PMC11617231
- DOI: 10.1016/j.rpth.2024.102610
External validation of the Leiden Thrombosis Recurrence Risk Prediction models (L-TRRiP) for the prediction of recurrence after a first venous thrombosis in the Heart and Vascular Health study
Abstract
Background: Long-term outcome after a first venous thromboembolism (VTE) might be optimized by tailoring anticoagulant treatment duration on individual risks of recurrence and major bleeding. The L-TRRiP models (A-D) were previously developed in data from the Dutch Multiple Environment and Genetic Assessment of Risk Factors for Venous thrombosis study to predict VTE recurrence.
Objectives: We aimed to externally validate models C and D using data from the United States Heart and Vascular Health (HVH) study.
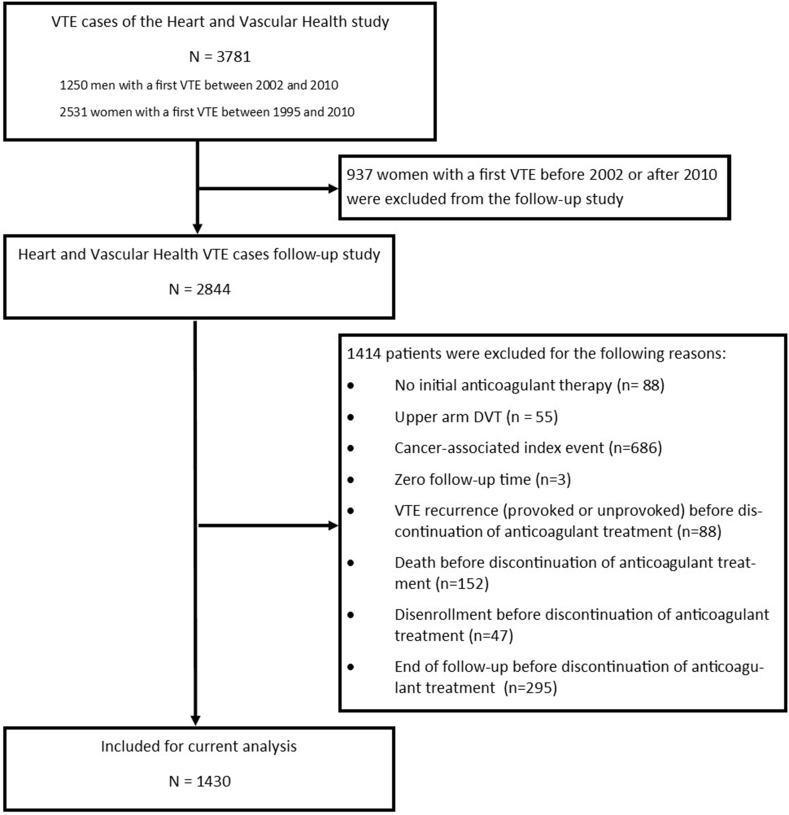
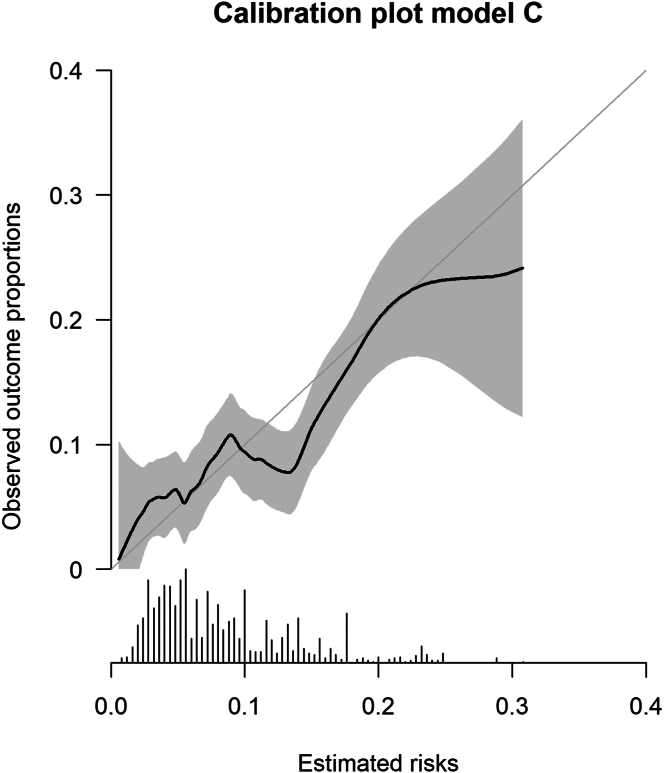
Methods: Data from participants with a first VTE who discontinued initial anticoagulant therapy were used to determine model performance. Missing data were imputed, and results were pooled according to Rubin's rules. To determine discrimination, Harrell's C-statistic was calculated. To assess calibration, the observed/expected (O/E) ratio was estimated, and calibration plots were created, in which we accounted for the competing risk of death. A stratified analysis based on age <70 or >70 years was performed.
Results: Of 1430 participants from the HVH study, 187 experienced an unprovoked VTE recurrence during follow-up. The C-statistics of L-TRRIP models C and D were 0.62 (95% CI, 0.56-0.67) and 0.61 (95% CI, 0.55-0.67), respectively. The O/E ratio (1.00; 95% CI, 0.84-1.17 and 1.09; 95% CI, 0.91-1.27, respectively) and calibration plots indicated good calibration. The discrimination was similar between participants <70 or >70 years, whereas overall calibration was lower in participants <70 years.
Conclusion: The L-TRRiP models showed moderate discrimination and good calibration in a different population and can be used to guide clinical decision making. To assess the added value in daily clinical practice, a management study is needed.
Keywords: anticoagulants; clinical decision rules; prognosis; validation study; venous thromboembolism.
© 2024 The Authors.
Figures
References
-
- Khan F., Rahman A., Carrier M., Kearon C., Weitz J.I., Schulman S., et al. Long term risk of symptomatic recurrent venous thromboembolism after discontinuation of anticoagulant treatment for first unprovoked venous thromboembolism event: systematic review and meta-analysis. BMJ. 2019;366:l4363. - PMC - PubMed
-
- Iorio A., Kearon C., Filippucci E., Marcucci M., Macura A., Pengo V., et al. Risk of recurrence after a first episode of symptomatic venous thromboembolism provoked by a transient risk factor: a systematic review. Arch Intern Med. 2010;170:1710–1716. - PubMed
-
- Khan F., Tritschler T., Kimpton M., Wells P.S., Kearon C., Weitz J.I., et al. Long-term risk for major bleeding during extended oral anticoagulant therapy for first unprovoked venous thromboembolism: a systematic review and meta-analysis. Ann Intern Med. 2021;174:1420–1429. - PubMed
-
- Burggraaf J.L.I., van Rein N., Klok F.A., Cannegieter S.C. How to predict recurrent venous thromboembolism and bleeding? A review of recent advances and their implications. Pol Arch Intern Med. 2023;133:16492. - PubMed
LinkOut - more resources
Full Text Sources
