

The global, regional, and national burden of urolithiasis in 204 countries and territories, 2000-2021: a systematic analysis for the Global Burden of Disease Study 2021
- PMID: 39640943
- PMCID: PMC11618031
- DOI: 10.1016/j.eclinm.2024.102924
The global, regional, and national burden of urolithiasis in 204 countries and territories, 2000-2021: a systematic analysis for the Global Burden of Disease Study 2021
Abstract
Background: Urolithiasis is a common urological problem that is associated with high morbidity. A comprehensive assessment of the non-fatal and fatal health trends of urolithiasis by age, sex, and geography over time is necessary to inform policy to control this surgically managed non-communicable disease.
Methods: This study was conducted using the standard GBD methodology and analytic tools. Cause-specific mortality rate (CSMR) was estimated using vital registration and verbal autopsy data and the Cause of Death Ensemble model (CODEm) modelling tool. CSMR estimates and incidence data from medical insurance claims and hospital discharges were analysed using a Bayesian meta-regression modelling tool, DisMod-MR 2.1, to estimate age-, sex-, and location-specific incidence of urolithiasis between 2000 and 2021. Disability-adjusted life-years (DALYs) were the sum of years of life lost (YLL) and years lived with disability (YLDs). YLLs due to urolithiasis were calculated by multiplying the estimated number of deaths by the standard life expectancy at the age of death. YLDs were estimated by multiplying the disability weight by the symptomatic proportion of urolithiasis cases. The Global Burden of Diseases study used de-identified data, approved by the University of Washington IRB (Study Number 9060).
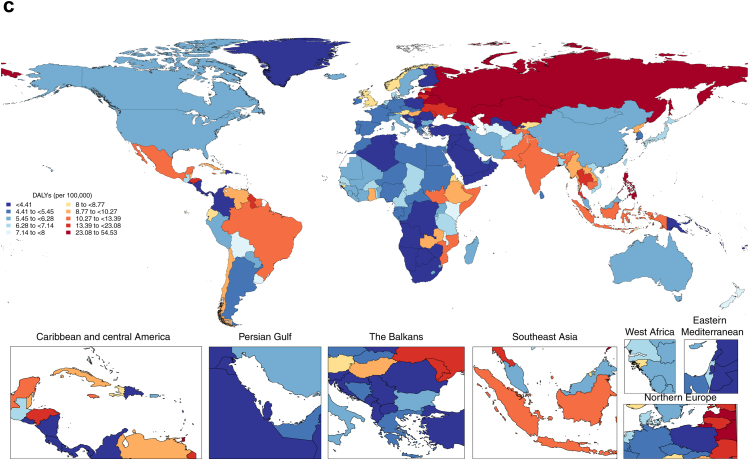
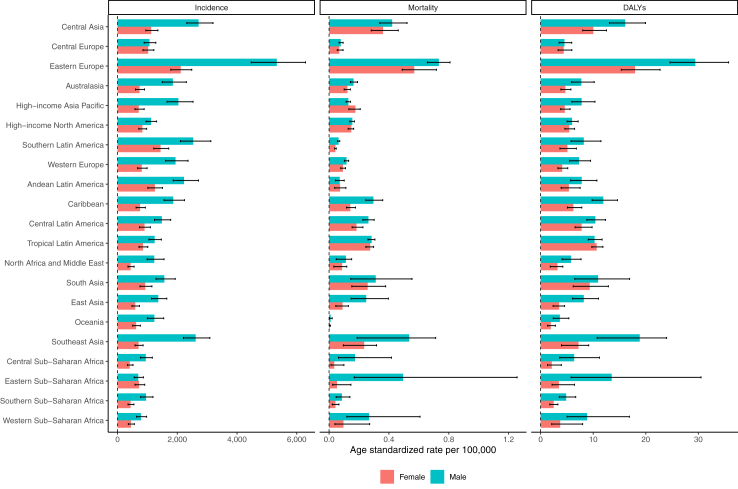
Findings: There were 106 million (95% UI 88.3-129.0) incident cases of urolithiasis in 2021, of which 67% were in men (71.1 million [59.4-86.2)]). The global number of incident cases, deaths, and DALYs increased by 26.7% (23.8-29.8), 60.3% (41.5-84.7), and 34.5% (24.6-47.3), respectively, between 2000 and 2021. The global age-standardised incidence rate of urolithiasis experienced a significant decrease of 17.5% (14.7-20.0), while the age-standardised DALYs rate saw a reduction of 15.1% (6.8-21.3). Twelve GBD regions showed declining trends in the age-standardised incidence rate of urolithiasis between 2000 and 2021, and the remaining nine GBD regions had an increasing trend of age-standardised rates of urolithiasis. A significant increase in the age-standardised incidence rate of urolithiasis was observed in Central America, Tropical Latin America, and the Caribbean regions, whereas notable decline was observed in east Asia, eastern Europe, central Europe, and high-income North America. It was observed that the global age-standardised death rate was less than 0.5 per 100,000 across all GBD regions and less than 1 per 100,000 across all SDI quintiles, with fairly stable global age-standardised death rates of urolithiasis between 2000 and 2021. The age-standardised incidence rate of urolithiasis was 837 (688-1034) in low SDI regions and 1443 (12,108-1734) in high-middle SDI regions. Furthermore, the age-standardised DALY rate showed a decreasing trend across all SDI quintiles over the same period: high-middle SDI (-28.9% [-34.4 to -23.0]), middle SDI (-22.6% [-30.5 to -10.9]), and low-middle SDI (-2.9% [-15.8 to 12.9]).
Interpretation: Global urolithiasis incidence and DALY rates have decreased, while the death rate has stabilised worldwide, showing significant variability among regions, SDI levels, and countries. This could be due to effective preventive measures c on urolithiasis risk factors, effective public health education, lifestyle changes, and early interventions and improved health care access at the global level. This analysis offers relevant insights into global, regional, and country-specific urolithiasis trends.
Funding: Bill & Melinda Gates Foundation.
Keywords: Disability adjusted life loss; Global burden of disease; Incidence; Nephrolithiasis; Urolithiasis.
© 2024 The Author(s).
Conflict of interest statement
S Bhaskar reports grants or contracts from the Japan Society for the Promotion of Science (JSPS), Japanese Ministry of Education, Culture, Sports, Science, and Technology (MEXT) and JSPS and the Australian Academy of Science; leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid, with Rotary District 9675, Sydney, Australia; Global Health & Migration Hub Community, Global Health Hub Germany, Berlin, Germany; PLOS One, BMC Neurology, Frontiers in Neurology, Frontiers in Stroke, Frontiers in Public Health, Journal of Aging Research, and BMC Medical Research Methodology; College of Reviewers, Canadian Institutes of Health Research, Government of Canada; World Headache Society, Bengaluru India; Cariplo Foundation, Milan, Italy; National Cerebral and Cardiovascular Center, Department of Neurology, Suita, Osaka, Japan; Cardiff University Biobank, Cardiff, UK, all outside the submitted work. B Bikbov reports grants or contracts from the European Commission, University of Rome, and Politecnico di Milano; supporting for attending meetings and/or travel from the European Renal Association; leadership or fiduciary roles in board, society, committee or advocacy groups, unpaid, with the International Society of Nephrology and the Western Europe Regional Board, International Society of Nephrology; and other support from Scientific-Tools.org, all outside the submitted work. I Ilic report support for the present manuscript from the Ministry of Education, Science, and Technological Development, Republic of Serbia (Project No. 175042, 2011–2023). M Ilic reports support for the present manuscript from the Ministry of Science, Technological Development, and Innovation, Republic of Serbia (Project No. 451-03-47/2023-01/200111). A-F A Mentis reports grants or contracts from ‘MilkSafe: A novel pipeline to enrich formula milk using omics technologies', a research co financed by the European Regional Development Fund of the European Union and Greek national funds through the Operational Program Competitiveness, Entrepreneurship and Innovation, under the call RESEARCH–CREATE–INNOVATE (project code: T2EDK-02222), as well as from ELIDEK (Hellenic Foundation for Research and Innovation, MIMS-860) (both outside of the present manuscript); payment or expert testimony as a peer-reviewer for FONDAZIONE CARIPLO, ITALY; Participation on a Data Safety Monitoring Board or Advisory Board as Editorial Board Member for “Systematic Reviews” journal, for “Annals of Epidemiology” journal, and as Associate Editor for “Translational Psychiatry”; stock or stock options on a family winery; other financial interests as a scientific officer as part of the BGI Group; outside the submitted work. A Ortiz reports grants to their institute from Sanofi and Catedra Mundipharma-UAM of diabetic kidney disease and the Catedra Astrazeneca-UAM of chronic kidney disease and electrolytes; consultancy or speaker fees Advicciene, Astellas, Astrazeneca, Amicus, Amgen, Fresenius Medical Care, GSK, Bayer, Sanofi-Genzyme, Menarini, Kyowa Kirin, Alexion, Idorsia, Chiesi, Otsuka, Novo-Nordisk and Vifor Fresenius Medical Care Renal Pharma; travel support from Advicciene, Astellas, Astrazeneca, Fresenius Medical Care, Boehringer-Ingelheim Bayer, Sanofi-Genzyme, Menarini, Chiesi, Otsuka, Sysmex; leadership or fiduciary role, unpaid, with Council ERA. SOMANE; all outside the submitted work. J A Singh reports consulting fees from ROMTech, Atheneum, Clearview healthcare partners, American College of Rheumatology, Yale, Hulio, Horizon Pharmaceuticals, DINORA, Frictionless Solutions, Schipher, Crealta/Horizon, Medisys, Fidia, PK Med, Two labs Inc., Adept Field Solutions, Clinical Care options, Putnam associates, Focus forward, Navigant consulting, Spherix, MedIQ, Jupiter Life Science, UBM LLC, Trio Health, Medscape, WebMD, and Practice Point communications; and the National Institutes of Health; Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events on the speakers bureau of Simply Speaking; Support for attending meetings and/or travel from OMERACT as a steering committee member; Participation on a Data Safety Monitoring Board or Advisory Board with the FDA Arthritis Advisory Committee; Leadership or fiduciary role in other board, society, committee or advocacy group, paid as a past steering committee member of the OMERACT, an international organization that develops measures for clinical trials and receives arm's length funding from 12 pharmaceutical companies, unpaid as Chair of the Veterans Affairs Rheumatology Field Advisory Committee, and unpaid as the Editor and Director of the UAB Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis; Stock or stock options in Atai life sciences, Kintara therapeutics, Intelligent Biosolutions, Acumen pharmaceutical, TPT Global Tech, Vaxart pharmaceuticals, Atyu biopharma, Adaptimmune Therapeutics, GeoVax Labs, Pieris Pharmaceuticals, Enzolytics Inc., Seres Therapeutics, Tonix Pharmaceuticals Holding Corp., Aebona Pharmaceuticals, and Charlotte's Web Holdings, Inc. and previously owned stock options in Amarin, Viking, and Moderna Pharmaceuticals; all outside the submitted work. A Zumla reports support for the present manuscript the Pan-African Network for Rapid Research, Response, Relief and Preparedness for Infectious Disease Epidemics (PANDORA-ID-NET) funded by the EDCTP–the EU Horizon 2020 Framework Programme, and is a recipient of the UK NIHR Senior Investigator Award, Mahathir Science Award, and EU-EDCTP Pascoal Mocumbi Prize Laureate.
Figures






References
-
- Pearle M.S., Jodi A., Antonelli J.A., Lotan Y. In: Campbell-Walsh Urology. 11th ed. Wein A.J., Kavoussi L.R., Partin A.W., Peters C.A., editors. Elsevier; Philadelphia: 2016. Urinary Lithiasis: etiology, epidemiology, and pathogenesis; pp. 1170–1291. 1600 John F. Kennedy Blvd.
-
- Chung M.J. Urolithiasis and nephrolithiasis. JAAPA. 2017;30(9):49–50. - PubMed
-
- Thakore P., Liang T.H. StatPearls. StatPearls Publishing; Treasure Island (FL): 2022. Urolithiasis.https://www.ncbi.nlm.nih.gov/books/NBK559101/ [Updated 2021 Jun 18] Available from:
-
- Sorokin I., Mamoulakis C., Miyazawa K., Rodgers A., Talati J., Lotan Y. Epidemiology of stone disease across the world. World J Urol. 2017;35(9):1301–1320. - PubMed
LinkOut - more resources
Full Text Sources
