

The diagnostic and prognostic value of soluble ST2 in Sepsis
- PMID: 39640977
- PMCID: PMC11617550
- DOI: 10.3389/fmed.2024.1487443
The diagnostic and prognostic value of soluble ST2 in Sepsis
Abstract
Objective: To determine the diagnostic and prognostic value of soluble suppression of tumorigenicity 2 (sST2) in patients with sepsis.
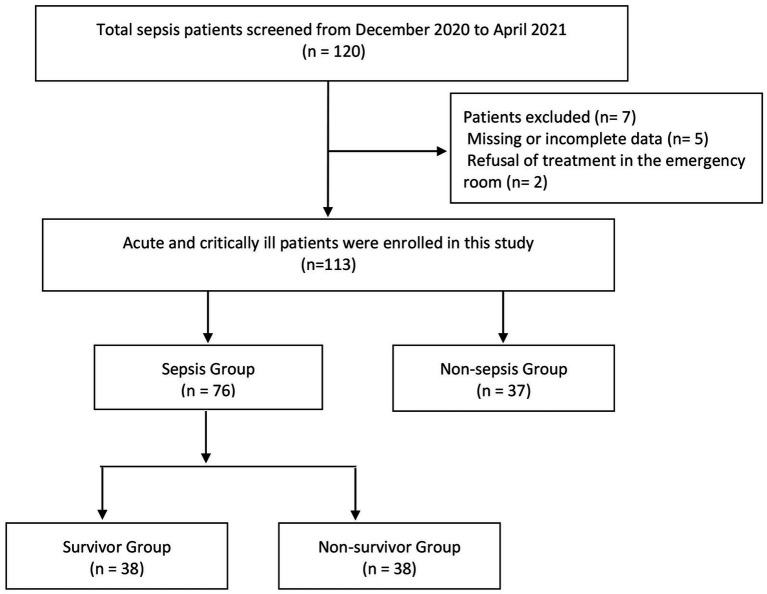
Methods: A total of 113 critically ill patients were enrolled at the emergency department of Beijing Chaoyang Hospital Jing Xi Branch. Venous blood levels of sST2 were measured using the AFIAS-6 dry fluorescence immunoassay analyzer. Based on Sepsis 3.0 criteria, patients were categorized into a sepsis group (76 cases) and a non-sepsis group (37 cases). The sepsis group was further divided into non-survivors (38 cases) and survivors (38 cases) based on 28-day survival outcomes. The vital signs, blood gas analysis, routine blood tests, liver and kidney function tests, procalcitonin (PCT), C-reactive protein (CRP), sST2, left ventricular ejection fraction (LVEF), and other basic characteristics of the patients were recorded. Further, the SOFA, qSOFA and APACHE II scores of each patient were calculated. Statistical analysis was performed using SPSS 25.0, including logistic regression and ROC curve analysis to assess prognostic factors.
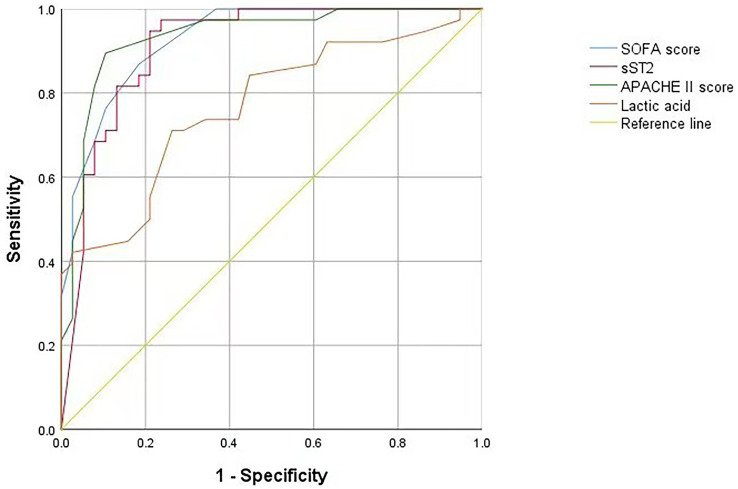
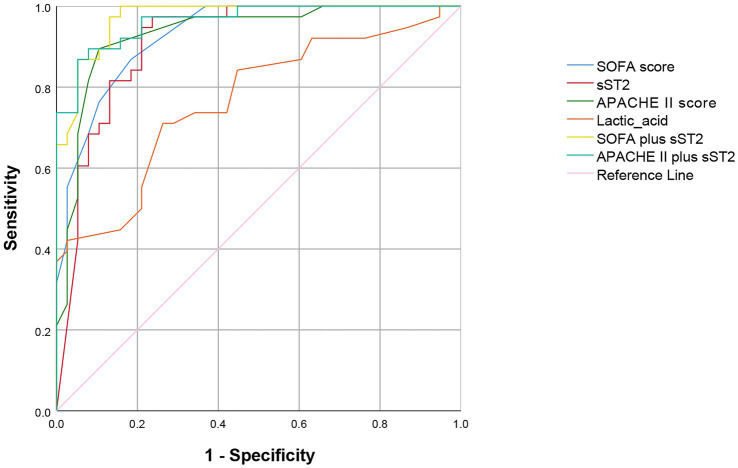
Results: The serum sST2 levels in the sepsis group (125.00 ± 60.32 ng/mL) were significantly higher than in the non-sepsis group (58.55 ± 39.03 ng/mL) (p < 0.05). The SOFA score (8.08 ± 2.88), APACHE II score (18.00 ± 4.72), blood sST2 levels (168.06 ± 36.75 ng/mL) and lactic acid levels (2.89 ± 3.28) in the non-survivor group were significantly higher than the survivor group (p < 0.05). Multiple logistic regression analysis showed that sST2, SOFA score, APACHE II score and lactic acid levels were independent risk factors for poor prognosis in patients with sepsis. The ROC curve analysis of the above indexes showed no significant differences between the AUC of sST2 (0.912) and the SOFA score (0.929) (z = 0.389, p = 0.697), or the APACHE II score (0.933) (z = 0.484, p = 0.627). However, there was a significant difference between the AUC of sST2 (0.912) and lactic acid levels (0.768) (z = 2.153, p = 0.030).
Conclusion: Blood levels of sST2 show a clinically diagnostic and prognostic value in sepsis. Further, sST2 shows a similar predictive ability as the SOFA and APACHE II scores in determining the prognosis of sepsis patients. However, sST2 has a higher predictive ability than lactic acid levels in determining prognosis in sepsis.
Keywords: APACHE II score; SOFA score; Sepsis; diagnosis; lactic acid; prognosis; soluble ST2.
Copyright © 2024 Ye, Wang, Hu, Zhang, Li, Xuan, Han, Qu, Yang, Yang, Wang and Wei.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous