

Cost-effectiveness of a Low-cost Educational Messaging and Prescription-fill Reminder Intervention to Improve Medication Adherence Among Individuals With Intellectual and Developmental Disability and Hypertension
- PMID: 39642010
- PMCID: PMC11617081
- DOI: 10.1097/MLR.0000000000001946
Cost-effectiveness of a Low-cost Educational Messaging and Prescription-fill Reminder Intervention to Improve Medication Adherence Among Individuals With Intellectual and Developmental Disability and Hypertension
Abstract
Background: Adults with intellectual and developmental disabilities (IDDs) have a similar prevalence of hypertension as the general population, but a higher rate of medication nonadherence at 50% compared with the average of 30%.
Objectives: To assess the cost-effectiveness of educational messaging and prescription-fill reminders to adults with IDD and hypertension and their helpers among Medicaid members in a randomized control trial.
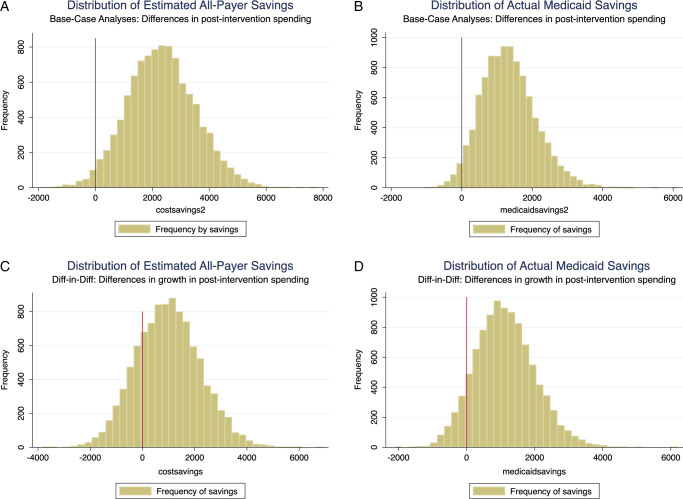
Research design: The authors calculated net cost savings by subtracting per-participant intervention costs from differences in spending between preintervention/postintervention cases versus controls. Using bootstrap samples, they assessed the probability of positive cost savings. They used quantile and logistic regression to examine which members contributed to the cost savings and to identify future high-cost members at baseline.
Subjects: Four hundred twelve members with IDD and their helpers were recruited from the South Carolina Medicaid agency in 2018.
Measures: Intervention costs were determined using labor and communication costs. Health expenditures were obtained from South Carolina's all-payer claims database, using actual Medicaid expenditures and total all-payer expenditures estimated with cost-to-charge ratios.
Results: The intervention, which cost $26.10 per member, saved $1008.02 in all-payer spending and $1126.42 in Medicaid payments per member, respectively, with 78% and 91% confidence. Cost savings occurred among members above the 85th percentile of spending, and those using the emergency department or inpatient services at least twice at baseline were predicted to be future high-cost members.
Conclusions: The intervention is cost-saving, and insurers can prospectively identify and target members who will likely benefit.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
B.C. serves as a member of the Board of Directors at Kaohsiung Medical University, a not-for-profit institution that provides medical education and medical care in Taiwan. He attends meetings quarterly, voting on issues related to the internal governance of the hospital and school with no overlap with the research at hand. The remaining authors declare no conflict of interest.
Figures
References
-
- Kochanek K Murphy S Xu J, et al. National vital statistics reports. National Center for Health Statistics. Center for Disease Control and Prevention, U.S. Department of Health and Human Services; 2019.
-
- de Winter CF, Bastiaanse LP, Hilgenkamp TI, et al. Cardiovascular risk factors (diabetes, hypertension, hypercholesterolemia and metabolic syndrome) in older people with intellectual disability: results of the HA-ID study. Res Dev Disabil. 2012;33:1722–1731. - PubMed
-
- Pharmacy Quality Alliance. PQA adherence measures. 2022. Accessed July 15, 2023. https://www.pqaalliance.org/adherence-measures
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
