

Mitigating and managing infection risk in adults treated with CAR T-cell therapy
- PMID: 39644015
- PMCID: PMC11706248
- DOI: 10.1182/hematology.2024000535
Mitigating and managing infection risk in adults treated with CAR T-cell therapy
Abstract
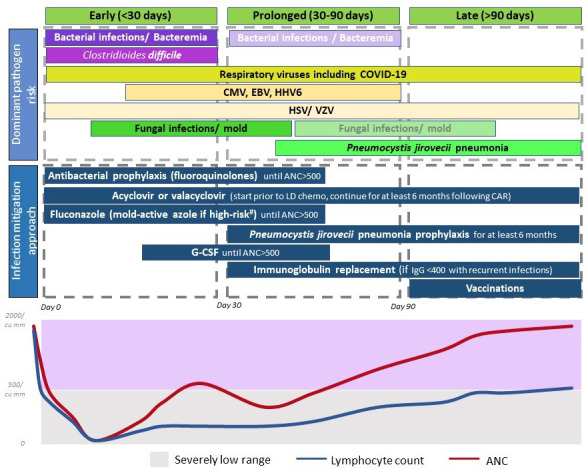
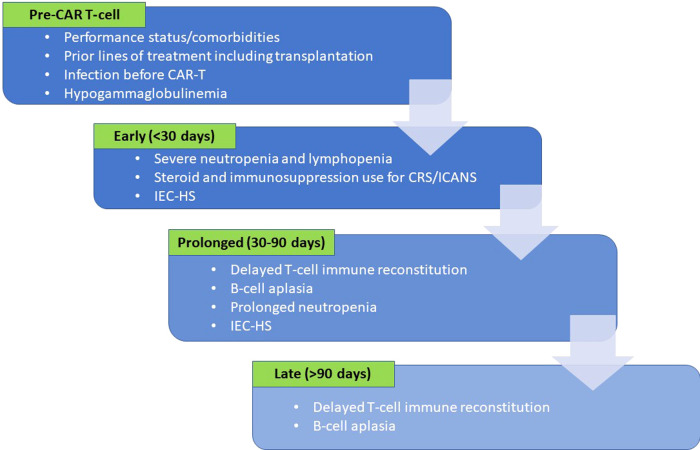
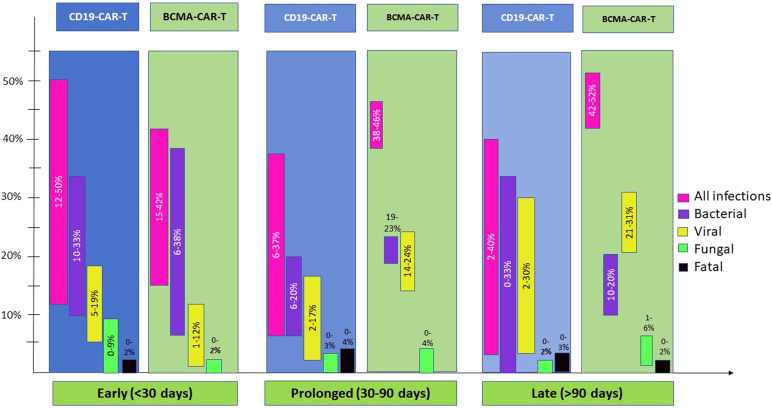
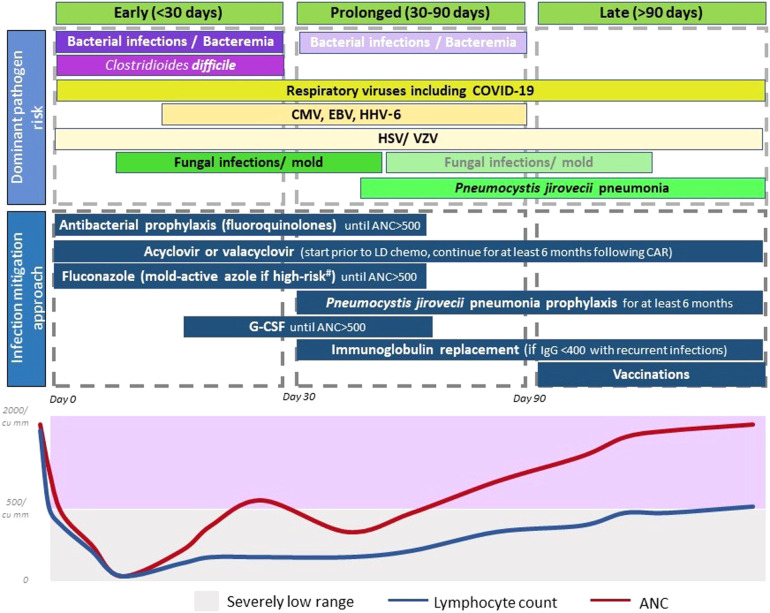
Chimeric antigen receptor T-cell therapy (CAR-T) has transformed the treatment paradigm of relapsed/refractory B-cell malignancies. Yet, this therapy is not without toxicities. While the early inflammation-mediated toxicities are now better understood, delayed hematopoietic recovery and infections result in morbidity and mortality risks that persist for months following CAR-T. The predisposition to infections is a consequence of immunosuppression from the underlying disease, prior therapies, lymphodepletion chemotherapy, delayed hematopoietic recovery, B-cell aplasia, and delayed T-cell immune reconstitution. These risks and epidemiology can vary over a post-CAR-T timeline of early (<30 days), prolonged (30-90 days), or late (>90 days) follow-up. Antibacterial, antiviral, and antifungal prophylaxis; growth factors and stem cell boost to expedite count recovery; immunoglobulin replacement therapy; and possibly revaccination programs are important prevention strategies to consider for infection mitigation. Assessment of risk factors, evaluation, and treatment for pathogen(s) prevalent in a particular time frame post-CAR-T are important clinical considerations in patients presenting with clinical features suggestive of infectious pathology. As more data emerge on the topic, personalized risk assessments to inform the type and duration of prophylaxis use and planning interventions will continue to emerge. Herein, we review our current approach toward infection mitigation while recognizing that this continues to evolve and that there are differences among practices stemming from data availability limitations.
Copyright © 2024 by The American Society of Hematology.
Conflict of interest statement
Nadeem Tabbara has no competing financial interests to declare.
M. Veronica Dioverti-Prono reports consultancy fees for Regeneron and research funding from AlloVir and Regeneron.
Tania Jain reports institutional research funding from CTI BioPharma, Kartos Therapeutics, Incyte, and Bristol Myers Squibb and advisory board participation with Bristol Myers Squibb, Incyte, AbbVie, CTI, Kite, Cogent Biosciences, Blueprint Medicines, Telios Pharma, Protagonist Therapeutics, Galapagos, TScan Therapeutics, Karyopharm, and MorphoSys.
Figures
References
-
- Kanate AS, Majhail N, DeFilipp Z, et al.. Updated indications for immune effector cell therapy: 2023 Guidelines from the American Society for Transplantation and Cellular Therapy. Transplant Cell Ther. 2023;29(10):594-597. - PubMed
-
- Jain T, Bar M, Kansagra AJ, et al.. Use of chimeric antigen receptor T cell therapy in clinical practice for relapsed/refractory aggressive B cell non-Hodgkin lymphoma: an expert panel opinion from the American Society for Transplantation and Cellular Therapy. Biol Blood Marrow Transplant. 2019;25(12):2305-2321. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials