

The burden of diseases, injuries, and risk factors by state in the USA, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021
- PMID: 39645376
- PMCID: PMC11694014
- DOI: 10.1016/S0140-6736(24)01446-6
The burden of diseases, injuries, and risk factors by state in the USA, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021
Erratum in
-
Department of Error.Lancet. 2025 Jan 25;405(10475):302. doi: 10.1016/S0140-6736(25)00105-9. Lancet. 2025. PMID: 39863369 Free PMC article. No abstract available.
Abstract
Background: The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2021 provides a comprehensive assessment of health and risk factor trends at global, regional, national, and subnational levels. This study aims to examine the burden of diseases, injuries, and risk factors in the USA and highlight the disparities in health outcomes across different states.
Methods: GBD 2021 analysed trends in mortality, morbidity, and disability for 371 diseases and injuries and 88 risk factors in the USA between 1990 and 2021. We used several metrics to report sources of health and health loss related to specific diseases, injuries, and risk factors. GBD 2021 methods accounted for differences in data sources and biases. The analysis of levels and trends for causes and risk factors within the same computational framework enabled comparisons across states, years, age groups, and sex. GBD 2021 estimated years lived with disability (YLDs) and disability-adjusted life-years (DALYs; the sum of years of life lost to premature mortality and YLDs) for 371 diseases and injuries, years of life lost (YLLs) and mortality for 288 causes of death, and life expectancy and healthy life expectancy (HALE). We provided estimates for 88 risk factors in relation to 155 health outcomes for 631 risk-outcome pairs and produced risk-specific estimates of summary exposure value, relative health risk, population attributable fraction, and risk-attributable burden measured in DALYs and deaths. Estimates were produced by sex (male and female), age (25 age groups from birth to ≥95 years), and year (annually between 1990 and 2021). 95% uncertainty intervals (UIs) were generated for all final estimates as the 2·5th and 97·5th percentiles values of 500 draws (ie, 500 random samples from the estimate's distribution). Uncertainty was propagated at each step of the estimation process.
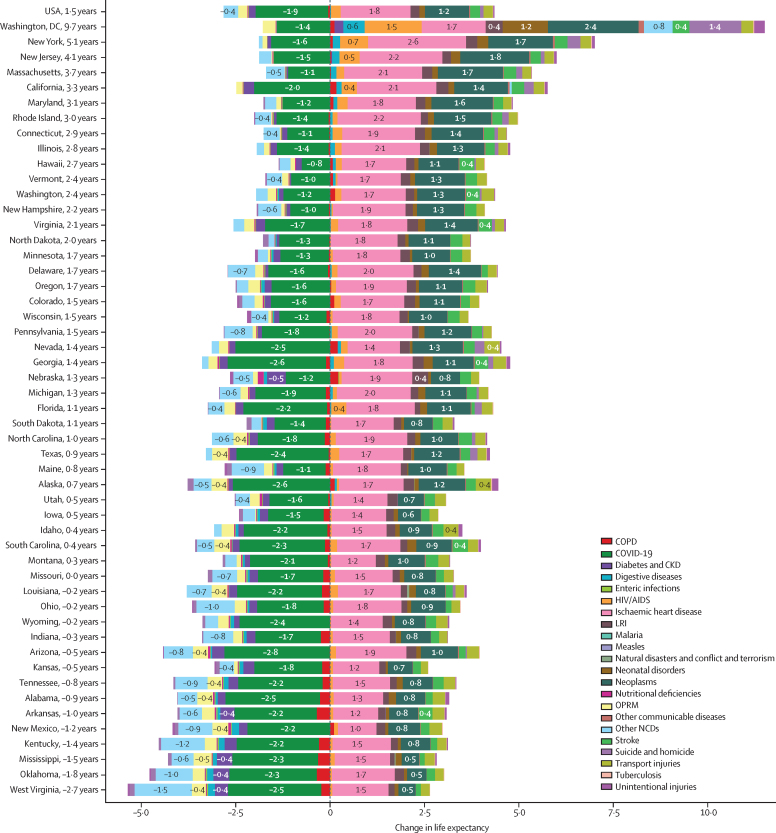
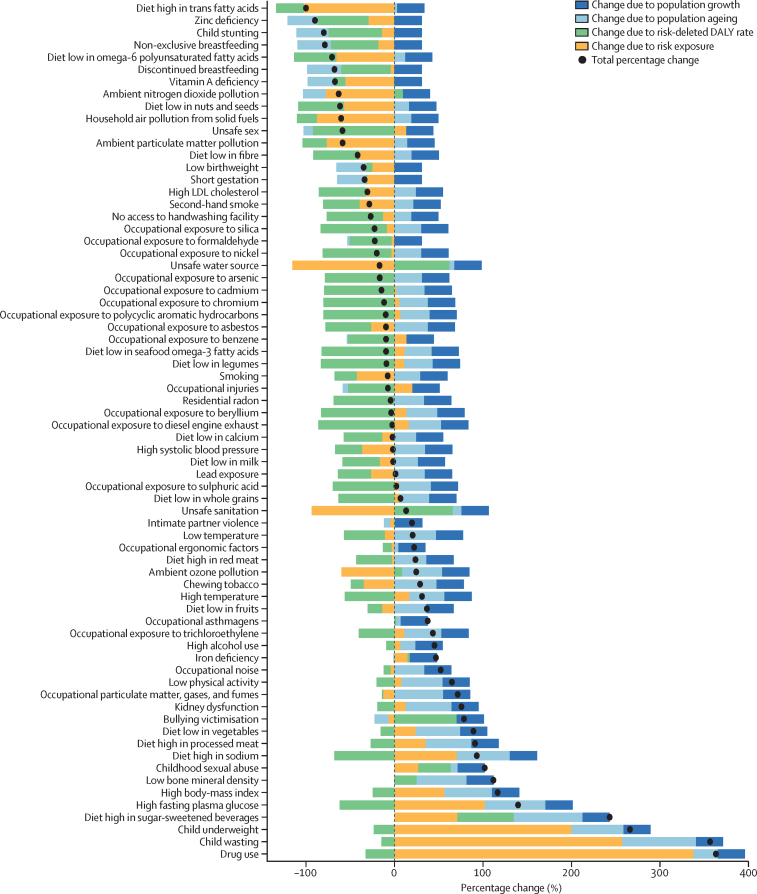
Findings: We found disparities in health outcomes and risk factors across US states. Our analysis of GBD 2021 highlighted the relative decline in life expectancy and HALE compared with other countries, as well as the impact of COVID-19 during the first 2 years of the pandemic. We found a decline in the USA's ranking of life expectancy from 1990 to 2021: in 1990, the USA ranked 35th of 204 countries and territories for males and 19th for females, but dropped to 46th for males and 47th for females in 2021. When comparing life expectancy in the best-performing and worst-performing US states against all 203 other countries and territories (excluding the USA as a whole), Hawaii (the best-ranked state in 1990 and 2021) dropped from sixth-highest life expectancy in the world for males and fourth for females in 1990 to 28th for males and 22nd for females in 2021. The worst-ranked state in 2021 ranked 107th for males (Mississippi) and 99th for females (West Virginia). 14 US states lost life expectancy over the study period, with West Virginia experiencing the greatest loss (2·7 years between 1990 and 2021). HALE ranking declines were even greater; in 1990, the USA was ranked 42nd for males and 32nd for females but dropped to 69th for males and 76th for females in 2021. When comparing HALE in the best-performing and worst-performing US states against all 203 other countries and territories, Hawaii ranked 14th highest HALE for males and fifth for females in 1990, dropping to 39th for males and 34th for females in 2021. In 2021, West Virginia-the lowest-ranked state that year-ranked 141st for males and 137th for females. Nationally, age-standardised mortality rates declined between 1990 and 2021 for many leading causes of death, most notably for ischaemic heart disease (56·1% [95% UI 55·1-57·2] decline), lung cancer (41·9% [39·7-44·6]), and breast cancer (40·9% [38·7-43·7]). Over the same period, age-standardised mortality rates increased for other causes, particularly drug use disorders (878·0% [770·1-1015·5]), chronic kidney disease (158·3% [149·6-167·9]), and falls (89·7% [79·8-95·8]). We found substantial variation in mortality rates between states, with Hawaii having the lowest age-standardised mortality rate (433·2 per 100 000 [380·6-493·4]) in 2021 and Mississippi having the highest (867·5 per 100 000 [772·6-975·7]). Hawaii had the lowest age-standardised mortality rates throughout the study period, whereas Washington, DC, experienced the most improvement (a 40·7% decline [33·2-47·3]). Only six countries had age-standardised rates of YLDs higher than the USA in 2021: Afghanistan, Lesotho, Liberia, Mozambique, South Africa, and the Central African Republic, largely because the impact of musculoskeletal disorders, mental disorders, and substance use disorders on age-standardised disability rates in the USA is so large. At the state level, eight US states had higher age-standardised YLD rates than any country in the world: West Virginia, Kentucky, Oklahoma, Pennsylvania, New Mexico, Ohio, Tennessee, and Arizona. Low back pain was the leading cause of YLDs in the USA in 1990 and 2021, although the age-standardised rate declined by 7·9% (1·8-13·0) from 1990. Depressive disorders (56·0% increase [48·2-64·3]) and drug use disorders (287·6% [247·9-329·8]) were the second-leading and third-leading causes of age-standardised YLDs in 2021. For females, mental health disorders had the highest age-standardised YLD rate, with an increase of 59·8% (50·6-68·5) between 1990 and 2021. Hawaii had the lowest age-standardised rates of YLDs for all sexes combined (12 085·3 per 100 000 [9090·8-15 557·1]), whereas West Virginia had the highest (14 832·9 per 100 000 [11 226·9-18 882·5]). At the national level, the leading GBD Level 2 risk factors for death for all sexes combined in 2021 were high systolic blood pressure, high fasting plasma glucose, and tobacco use. From 1990 to 2021, the age-standardised mortality rates attributable to high systolic blood pressure decreased by 47·8% (43·4-52·5) and for tobacco use by 5·1% (48·3%-54·1%), but rates increased for high fasting plasma glucose by 9·3% (0·4-18·7). The burden attributable to risk factors varied by age and sex. For example, for ages 15-49 years, the leading risk factors for death were drug use, high alcohol use, and dietary risks. By comparison, for ages 50-69 years, tobacco was the leading risk factor for death, followed by dietary risks and high BMI.
Interpretation: GBD 2021 provides valuable information for policy makers, health-care professionals, and researchers in the USA at the national and state levels to prioritise interventions, allocate resources effectively, and assess the effects of health policies and programmes. By addressing socioeconomic determinants, risk behaviours, environmental influences, and health disparities among minority populations, the USA can work towards improving health outcomes so that people can live longer and healthier lives.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests S Ashina reports consulting fees from AbbVie, Allegan, Eli Lilly and Company, Lundbeck, Theranica, Linpharma, Satsuma, and Pfizer; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Teva, Eli Lilly, and Lundbeck; leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid with HIS as a Member of the Educational Committee and as a Trustee of the IHS Board; outside the submitted work. T Bärnighausen reports grants or contracts from the National Institutes of Health, Alexander von Humboldt Foundation, German National Research Foundation (DFG), the European Union, German Ministry of Education and Research, German Ministry of the Environment, Wellcome, and KfW; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from PLOS; participation on a Data Safety Monitoring Board or Advisory Board for NIH-funded research projects in Africa on Climate Change and Health; Stock or stock options in CHEERS (an SME focusing on approaches to measure climate change and health-related variables in population cohorts); outside the submitted work. M L Bell reports grants or contracts from the US EPA, NIH, High Tide Foundation, Health Effects Institute, Yale Women Faculty Forum, Environmental Defense Fund, Wellcome Trust Foundation, Yale Climate Change and Health Center, Robert Wood Johnson Foundation, and the Hutchinson Postdoctoral Fellowship; Consulting fees from Clinique, ToxiMap, and SciQuest; honoraria for lectures, presentations, speakers bureaus from the Colorado School of Public Health, Duke University, Univ. of Texas, Data4Justice, Korea University, Organization of Teratology Information Specialists, UPenn, Boston University, Honorarium for editorial duties from IOP Publishing, honorarium for grant review from NIH, Health Canada, EHS, PAC-10, UKRI, AXA, Research Fund Fellowship, University of Texas, honorarium for external advisory committees from Harvard University and the University of Montana, Honorarium for online survey/workshop from SciQuest, and payment for teaching/researching for Korea University; Support for attending meetings and/or travel from Colorado School of Public Health, University of Texas, Duke University, Boston University, UPenn, Harvard University, American Journal of Public Health, Columbia Univ., Harvard, CMAS conference, Nature Conference; Leadership or fiduciary role in other board, society, committee or advisory group unpaid with the Fifth National Climate Assessment, Lancet Countdown, Johns Hopkins EHE Advisory Board, Harvard external advisory committee for training grants, WHO Global Air Pollution and Health Technical Advisory Group, National Academies Panels and Committees, and paid with the US EPA Clean Air Scientific Advisory Committee (CASAC); all outside the submitted work. A Beloukas reports grants or contracts from Gilead and GSK; Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Gilead and GSK; Support for attending meetings and/or travel from Gilead and GSK; and Receipt of equipment, materials, drugs, medical writing, gifts or other services from Cepheid for a research project; outside the submitted work. S Bhaskar reports grants or contracts from the Japan Society for the Promotion of Science (JSPS), Japanese Ministry of Education, Culture, Sports, Science and Technology (MEXT) and from The Australian Academy of Science; leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid as the visiting director in the department of neurology at the National Cerebral and Cardiovascular Center, Suita (Osaka, Japan), district chair of diversity, equity and inclusion at the Rotary District 9675, chair and manager of the Global Health and Migration Hub Community (Berlin, Germany), an editorial member of PLOS One, BMC Neurology, Frontiers in Neurology, Frontiers in Stroke, Frontiers in Aging, Frontiers in Public Health & BMC Medical Research Methodology, a member of the College of Reviewers (Canadian Institutes of Health Research, Government of Canada), a member of the scientific review committee at Cardiff University Biobank (Cardiff, UK), an export advisor and reviewer with the Cariplo Foundation (Milan, Italy), Pandemic Health System Resilience Program (REPROGRAM) Consortium as the global chair; outside the submitted work. E J Boyko reports payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from the Korean Diabetes Association, the Diabetes Association of the ROC (Taiwan), the American Diabetes Association, and the International Society for the Diabetic Foot; Support for attending meetings and/or travel from the Korean Diabetes Association, the Diabetes Association of the ROC (Taiwan), and the International Society for the Diabetic Foot; outside the submitted work. S Cortese reports grants or contracts NIHR; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from the ACAMH, BAP, and Medice; Support for attending meetings and/or travel from Medice; Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid with Eunethydis; outside the submitted work. S Das reports leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid as the Program Chair of Association for Diagnostic and Laboratory Medicine India Section (Voluntary Role) and as a Member of Women in Global Health; outside the submitted work. L Degenhardt reports grants or contracts from Indivior; outside the submitted work. I Filip reports other financial or non-financial interests with Avicenna Medical and Clinical Institute; outside the submitted work. A Guha reports grants or contracts from the American Heart Association and the Department of Defense; Consulting feeds from Pfizer and Novartis; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid on the health equity task force of ZERO Prostate Cancer; outside the submitted work. V-A Lioutas reports grants or contracts from the NIH and the Alzheimer's Association; Consulting feeds from QMetis and Mindray; Support for attending meetings and/or travel from the World Stroke Organization; outside the submitted work. R Liu reports grants or contracts from National Institute of Mental Health grant #s: R01 MH115905, RF1 MH120830, R01 MH124899, R21 MH130767 (awarded to Massachusetts General Hospital); Consulting fees from Relmada Therapeutics; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Miami International Child and Adolescent Mental Health Conference, Massachusetts General Hospital, University of California (San Francisco); Support for attending meetings and/or travel from the American Foundation for Suicide Prevention; Participation on a Data Safety Monitoring Board or Advisory Board for the University of Pennsylvania (Chair for DSMB), University of Minnesota, and Massachusetts General Hospital; outside the submitted work. R V Martin reports support for the present manuscript from a NASA Grant; Grants or contracts from the Clean Air Fund; outside the submitted work. S A Meo reports grants or contracts from the Deputyship for Research and Innovation, Ministry of Education in Saudi Arabia (FKSUOR3-4-8); outside the submitted work. S K Panda reports support for the present manuscript from Siksha 'O’ Anusandhan (Deemed to be University); Grants or contracts from DST-GOVT OF ODISHA (Letter number 3444/ST); payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Utkal University; outside the submitted work. M Pigeolet reports grants or contracts from The Belgian Kids’ Fund for Pediatric Research; outside the submitted work. A Radfar reports other financial or non-financial interests in Avicenna Medical and Clinical Research Institute; outside the submitted work. A Rane reports stock or stock options in Agios Pharmaceuticals; outside the submitted work. N Scarmeas reports grants or contracts with Novo Nordisc; Participation on a Data Safety Monitoring Board or Advisory Board with the Multicultural Health Diet to Reduce Cognitive Decline & AD Risk, Primus AD, Albert Einstein College of Medicine (NIH funded study) as the chair of the data safety monitoring board, and on the data safety monitoring board of the Public Private funded Phase II Study in Germany; outside the submitted work. A Sharifan reports leadership or fiduciary role in other board, society, committee or advocacy group, unpaid as a steering member of Cochrane; Reciept of equipment, materials, drugs, medical writing, gifts or other services from Elsevier and Cochrane; outside the submitted work. V Shivarov reports patents planned, issued, or pending with the Bulgarian Patent Office; Stock or stock options in ICON Plc; and financial interests in Icon Plc (salary); outside the submitted work. S J Tromans reports grants or grant contracts from the 2023 Adult Psychiatric Morbidity Survey team, collecting epidemiological data on community-based adults living in England (this is a contracted study from NHS Digital, via the Department of Health and Social Care); leadership or fiduciary role in other board, society, committee or advocacy group, unpaid as the Academic Secretary for the Neurodevelopmental Psychiatry Special Interest Group at the Royal College of Psychiatrists; Editorial Board Member for BMC Psychiatry, Advances in Autism, Advances in Mental Health and Intellectual Disability, and Progress in Neurology and Psychiatry; outside the submitted work. M Zielińska reports other financial interests in AstraZeneca as an employee; outside the submitted work. All other authors declare no competing interests.
Figures






Comment in
-
The US health-care paradox: lifting the veil.Lancet. 2024 Dec 7;404(10469):2244-2246. doi: 10.1016/S0140-6736(24)02416-4. Lancet. 2024. PMID: 39645372 No abstract available.
References
-
- GBD 2021 Demographics Collaborators Global age-sex-specific mortality, life expectancy, and population estimates in 204 countries and territories and 811 subnational locations, 1950–2021, and the impact of the COVID-19 pandemic: a comprehensive demographic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403:1989–2056. - PMC - PubMed
-
- Lantz PM, House JS, Lepkowski JM, Williams DR, Mero RP, Chen J. Socioeconomic factors, health behaviors, and mortality: results from a nationally representative prospective study of US adults. JAMA. 1998;279:1703–1708. - PubMed
-
- Centers for Disease Control and Prevention Ten great public health achievements—United States, 2001-2010. JAMA. 2011;306:36–38. - PubMed
-
- GBD 2021 Diseases and Injuries Collaborators Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403:2133–2161. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
