

This is a preprint.
HUMAN ALVEOLAR MACROPHAGE FUNCTION IS IMPAIRED IN TUBERCULOSIS CONTACTS WITH DIABETES
- PMID: 39649174
- PMCID: PMC11623777
- DOI: 10.21203/rs.3.rs-5489046/v1
HUMAN ALVEOLAR MACROPHAGE FUNCTION IS IMPAIRED IN TUBERCULOSIS CONTACTS WITH DIABETES
Abstract
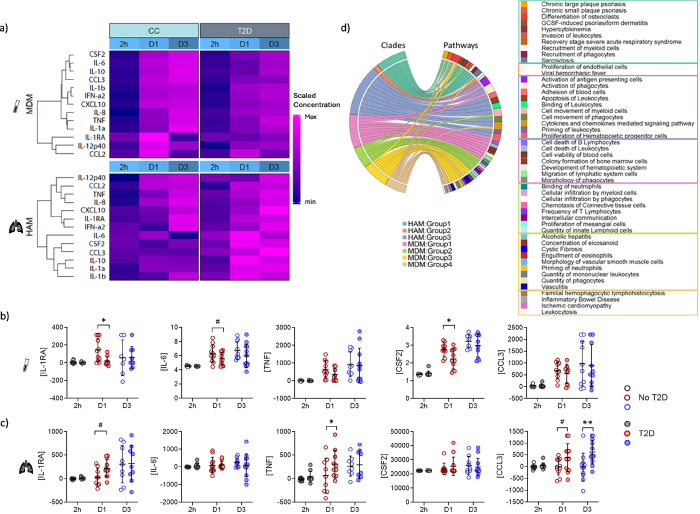
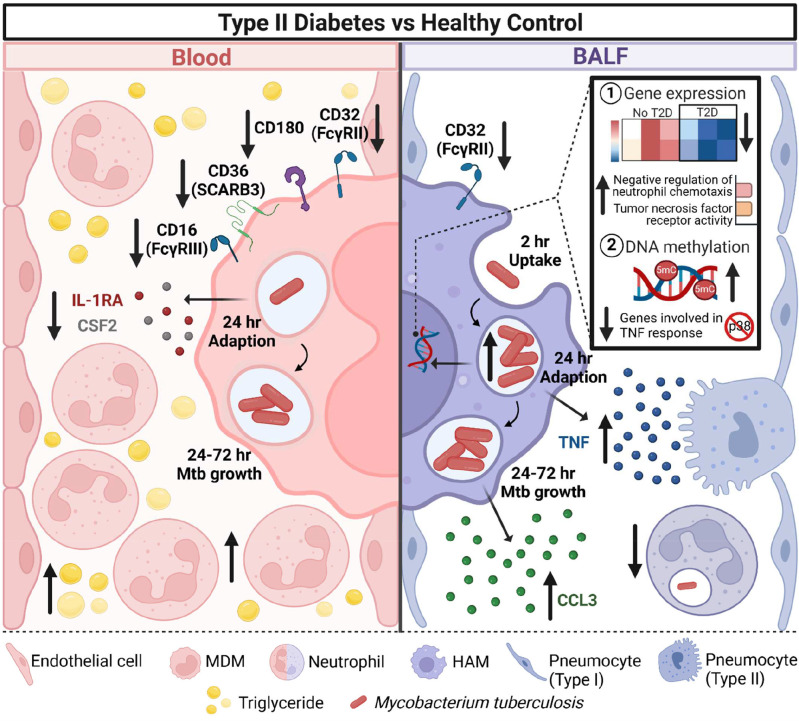
Type 2 diabetes (T2D) increases susceptibility to tuberculosis (TB) with the underlying mechanisms remaining unknown. To determine whether immune dysfunction in the lung contributes to TB susceptibility, we obtained paired human alveolar macrophages (HAMs) and monocyte-derived macrophages (MDMs) from TB-exposed individuals with/without T2D. Upon infection with Mycobacterium tuberculosis (M.tb), T2D-HAMs had more M.tb growth and produced more TNF. There were fewer neutrophils in the bronchoalveolar lavage of T2D patients which was inversely correlated with M.tb growth. Both T2D-HAMs and MDMs expressed less CD32, with T2D patients having fewer M1-like MDMs. T2D-MDMs produced less IL-1RA and CSF2. Overall M.tb-induced gene expression was delayed in T2D-HAMs, but genes involved in negative regulation of neutrophil migration were upregulated. T2D-HAM DNA was hypermethylated compared to control HAMs, however genes linked to TNF signalling were hypomethylated. We show here the first in-depth analysis of T2D-HAMs providing an explanation for more severe TB in T2D patients.
Keywords: alveolar macrophages; bronchoalveolar lavage; monocyte derived macrophages; mycobacterial growth; tuberculosis; type 2 diabetes.
Conflict of interest statement
CONFLICT OF INTEREST The authors declare no conflict of interest.
Figures






References
-
- World Health Organisation. Global Tuberculosis Report. 2023;https://www.who.int/teams/global-tuberculosis-programme/tb-reports/globa... .
-
- Noubiap JJ, Nansseu JR, Nyaga UF, Nkeck JR, Endomba FT, Kaze AD, et al. Global prevalence of diabetes in active tuberculosis: a systematic review and meta-analysis of data from 2ꞏ3 million patients with tuberculosis. Lancet Glob Health. 2019;7(4):e448–e60. - PubMed
-
- International Diabetes Federation. IDF Diabetes Atlas Tenth Edition. 2021;Accessed 29 April 2020(https://diabetesatlas.org/atlas/tenth-edition/).
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
