

This is a preprint.
Dihydroartemisinin-piperaquine versus sulfadoxine-pyrimethamine for intermittent preventive treatment of malaria in pregnancy: a systematic review and individual participant data meta-analysis
- PMID: 39649586
- PMCID: PMC11623747
- DOI: 10.1101/2024.11.23.24315401
Dihydroartemisinin-piperaquine versus sulfadoxine-pyrimethamine for intermittent preventive treatment of malaria in pregnancy: a systematic review and individual participant data meta-analysis
Update in
-
Dihydroartemisinin-piperaquine versus sulfadoxine-pyrimethamine for intermittent preventive treatment of malaria in pregnancy: a systematic review and individual participant data meta-analysis.EClinicalMedicine. 2025 Apr 29;83:103202. doi: 10.1016/j.eclinm.2025.103202. eCollection 2025 May. EClinicalMedicine. 2025. PMID: 40370584 Free PMC article.
Abstract
Background: High-grade Plasmodium falciparum resistance to sulfadoxine-pyrimethamine in East and Southern Africa has prompted numerous trials evaluating intermittent preventive treatment in pregnancy (IPTp) with dihydroartemisinin-piperaquine as an alternative to sulfadoxine-pyrimethamine.
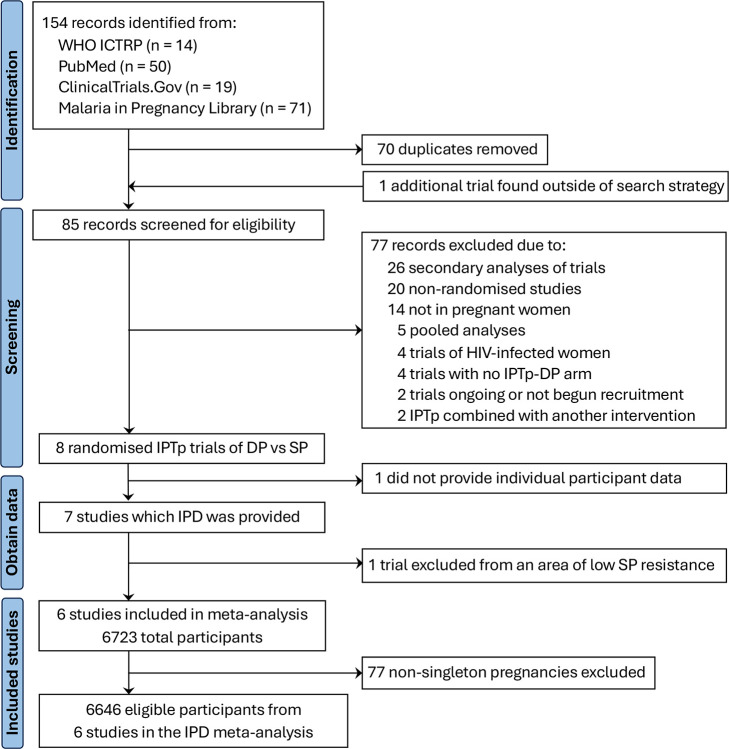
Methods: We conducted individual participant data meta-analyses of randomised trials comparing IPTp with dihydroartemisinin-piperaquine to sulfadoxine-pyrimethamine on maternal, birth, and infant outcomes. We searched the WHO International Clinical Trials Registry Platform, ClinicalTrials.Gov, PubMed, and the Malaria in Pregnancy Consortium Library. Eligible trials enrolled HIV-uninfected pregnant women, followed participants to delivery, included participants with no prior IPTp use during the current pregnancy, and were conducted in areas with high-level parasite resistance to sulfadoxine-pyrimethamine (i.e., PfDHPS 540E≥90% and/or 581G>0%). Only singleton pregnancies were analysed. Meta-analyses used a two-stage approach: first, study-specific estimates were generated and then pooled using a random-effects model. Gravidity subgroup analyses were performed. Causal mediation analyses were used to investigate the maternal mechanisms underlying the effect of IPTp regimens on birth outcomes. The meta-analysis is registered in PROSPERO (CRD42020196127).
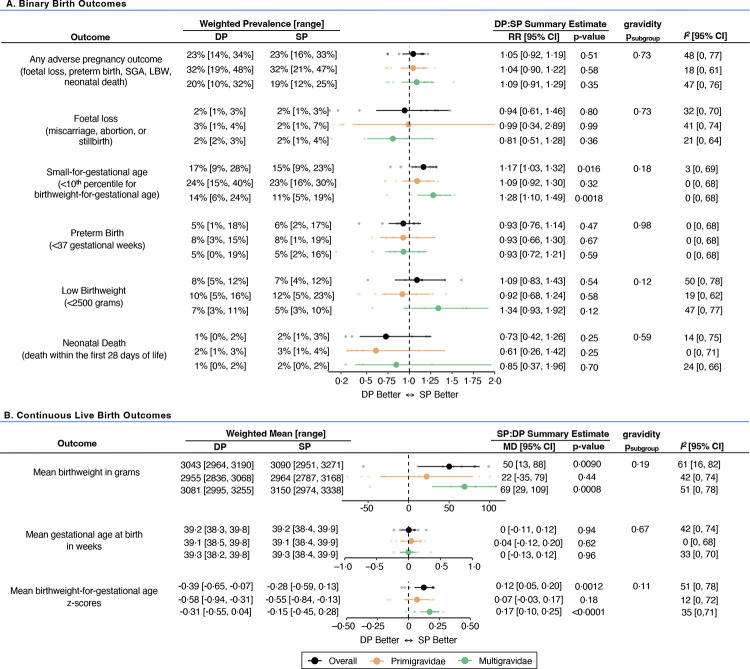
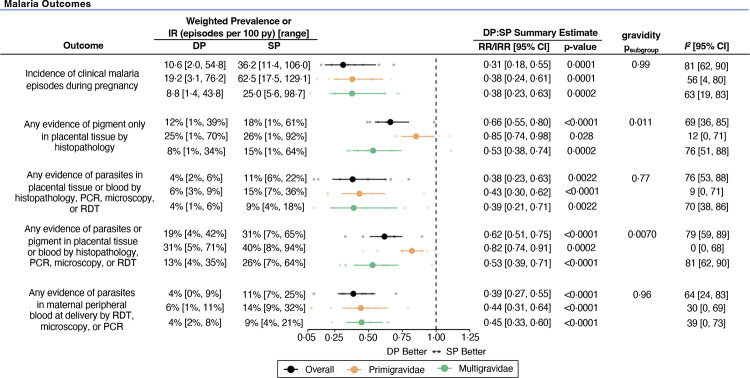
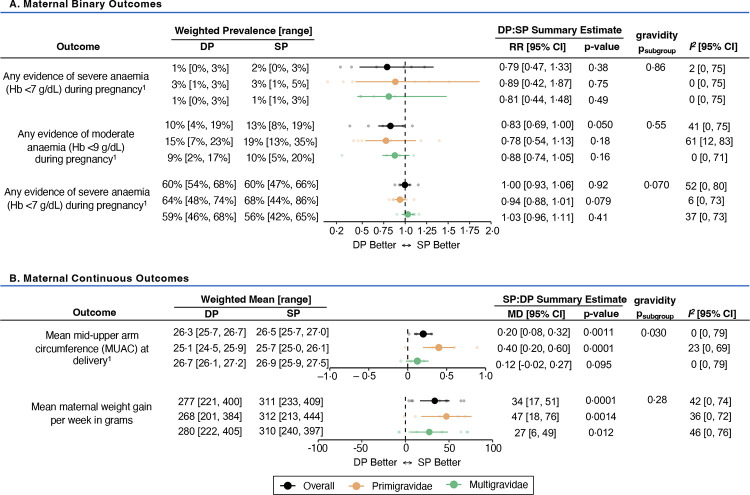
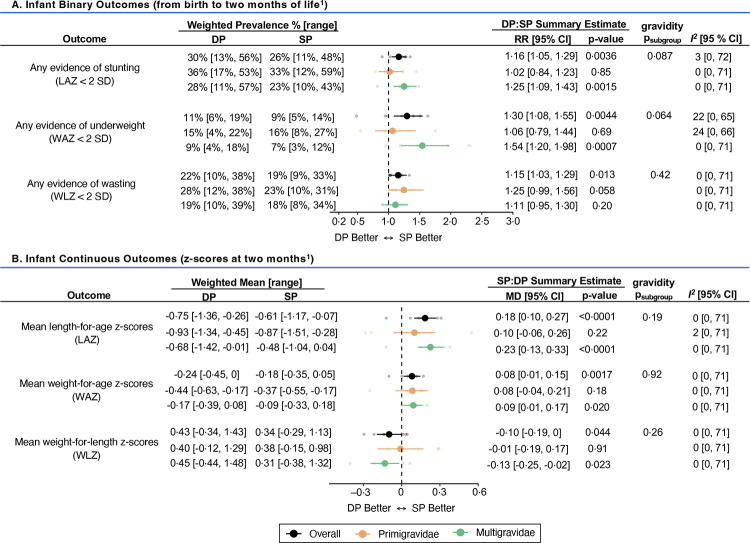
Findings: Of 85 screened records, six trials (one multi-country trial) contributed data on 6646 pregnancies. Compared to sulfadoxine-pyrimethamine, dihydroarteminsinin-piperaquine was associated with a 69% [95% CI: 45%-82%] lower incidence of clinical malaria during pregnancy, a 62% [37%-77%] lower risk of placental parasitaemia, and a 17% [0%-31%] lower incidence of moderate maternal anaemia (Hb<9 g/dL). In contrast, sulfadoxine-pyrimethamine was associated with higher mean weekly maternal weight gain (34 grams/week [17-51]). There were no statistically significant differences in the composite adverse pregnancy outcome between the two IPTp regimens (RR=1·05 [95% CI: 0·92-1·19]; I 2=48%), although the risk of small-for-gestational-age was 15% [3%-24%] lower in the sulfadoxine-pyrimethamine arm. Among multigravidae, participants of the sulfadoxine-pyrimethamine arm were 20% [8%-30%] and 35% [17%-49%] less likely to have stunted and underweight infants by two months compared to the dihydroartemisinin-piperaquine arm. Infant wasting by two months was 13% [3%-22%] lower in the sulfadoxine-pyrimethamine arm, regardless of gravidity. Mediation analyses indicated that 15% [0%-19%] of sulfadoxine-pyrimethamine's superior effect on reducing small-for-gestational-age risk was mediated by its greater impact on gestational weight gain.
Interpretation: In areas of high P. falciparum sulfadoxine-pyrimethamine resistance, dihydroartemisin-inpiperaquine is a more efficacious antimalarial than sulfadoxine-pyrimethamine. However, replacing sulfadoxine-pyrimethamine with dihydroartemisinin-piperaquine alone will not result in better maternal, birth, or infant outcomes. It could increase the risk of SGA, since much of the effect of sulfadoxine-pyrimethamine may be exerted through non-malarial mechanisms. Future research evaluating the alternative strategies for IPTp are needed, including with the combination of sulfadoxine-pyrimethamine and dihydroartemisinin-piperaquine.
Funding: This work was supported by the Bill and Melinda Gates Foundation and Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Keywords: Plasmodium falciparum; antimalarial resistance; dihydroartemisinin-piperaquine; foetal growth; intermittent preventive treatment in pregnancy; malaria; meta-analysis; non-malarial effects; sulfadoxine-pyrimethamine.
Conflict of interest statement
Declaration of interests All authors declare no competing interests.
Figures
References
-
- Desai M, Ter Kuile FO, Nosten F, et al. Epidemiology and burden of malaria in pregnancy. Lancet Infect Dis 2007; 7(2): 93–104. - PubMed
-
- World Health Organization. World Malaria Report 2023. Geneva, Switzerland: World Health Organization; 2024.
-
- World Health Organization. WHO guidelines for malaria, 3 June 2022: World Health Organization, 2022.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources