

Clinical Outcomes of Transjugular Intrahepatic Portosystemic Shunt Among Cirrhosis Patients With Recurrent Esophageal Variceal Bleeding
- PMID: 39651005
- PMCID: PMC11621572
- DOI: 10.7759/cureus.73101
Clinical Outcomes of Transjugular Intrahepatic Portosystemic Shunt Among Cirrhosis Patients With Recurrent Esophageal Variceal Bleeding
Abstract
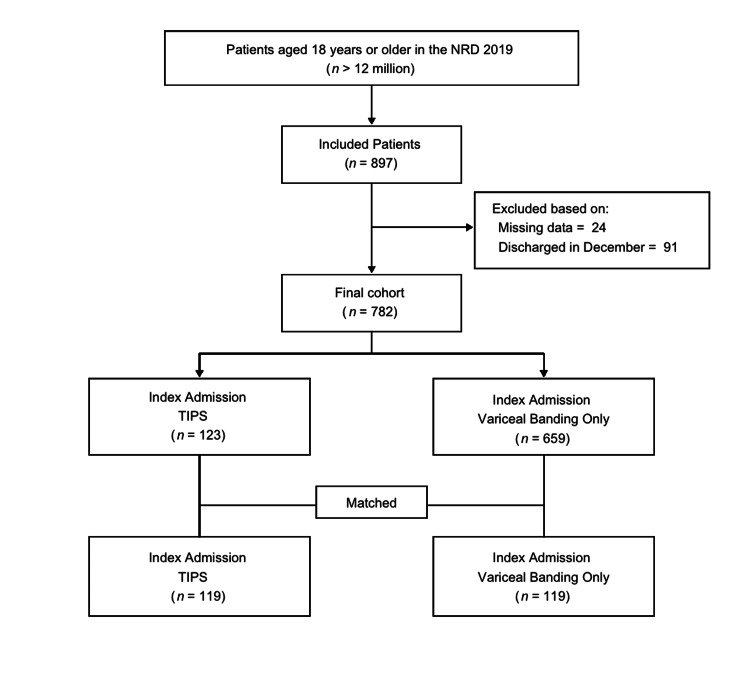
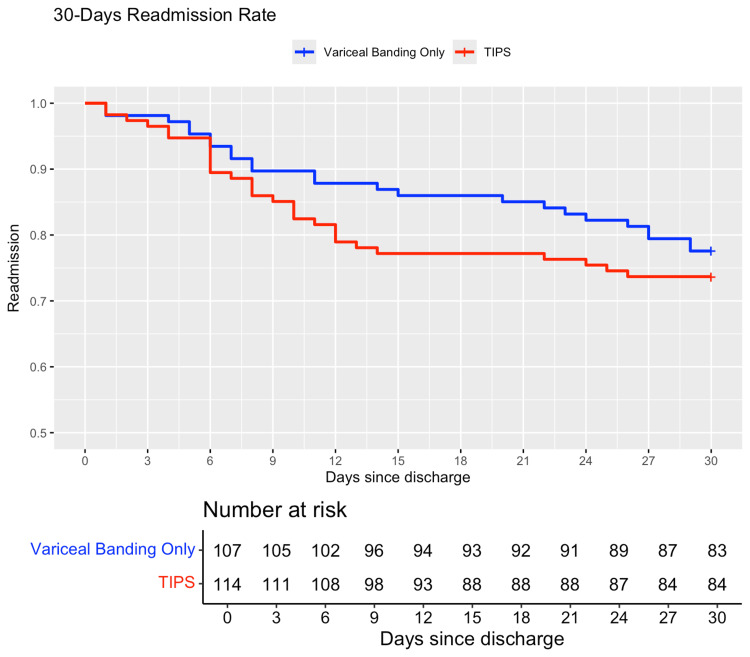
Background Transjugular intrahepatic portosystemic shunt (TIPS) has been shown to reduce the risk of rebleeding among patients with recurrent esophageal variceal bleeding. However, the impact of TIPS on survival remains uncertain. This study took on this challenge to determine if TIPS has any impact on all-cause inpatient mortality during the hospitalization in which it is performed and if it impacts all-cause 30-day readmission rates when compared to patients who only undergo esophageal variceal banding (EVB) for recurrent esophageal variceal bleeding. Methods This was a retrospective cohort study using the Healthcare Cost and Utilization Project - National Readmission Database 2019. All adult patients who had a diagnosis of cirrhosis, were hospitalized once for esophageal variceal bleeding requiring EVB in 2019, and then were hospitalized again later in the year for recurrent esophageal variceal bleeding requiring either TIPS or EVB were included. This second hospitalization in which patients either received TIPS or EVB only was considered as the index hospitalization. Patients with missing data and patients who were discharged in December were excluded. The primary outcome was all-cause 30-day readmission rates among patients who either received TIPS or EVB only. The secondary outcomes included: (i) incidence of all-cause inpatient mortality; and (ii) length of hospital stay during index hospitalization. Patients who underwent TIPS were matched with patients who underwent EVB only on age, sex, and baseline comorbidities. After propensity score matching, survival analysis was performed to compare the all-cause 30-day readmission rates after the index hospitalization, between patients who either received TIPS or EVB only during the index hospitalization. χ2 test was used to compare the inpatient mortality. As the data did not have a normal distribution, the Wilcoxon signed-rank test was used to compare the length of index hospitalization between patients who either received TIPS or EVB only. The alpha criterion was set at 0.05 for all statistical tests. Results This study found no difference in all-cause 30-day readmission rates between patients who underwent either TIPS or EVB only for recurrent esophageal variceal bleeding (hazard ratio: 1.24, 95%CI: 0.73-2.12, P = 0.4). In the exploratory analysis, it was noted that the rate of recurrent esophageal variceal bleeding, among patients who were readmitted within 30 days was lower in the TIPS group (13.3%) when compared to the EVB group (50%) with a risk ratio of 0.27 (95%CI: 0.10-0.72, P = 0.003). Although it was not statistically significant, the inpatient mortality rate during the index hospitalization appeared to be lower in the TIPS group when compared to the EVB group (4.2% vs 10.08%, respectively). Patients who underwent TIPS were hospitalized three days longer than patients who underwent EVB only. Conclusion TIPS does not reduce all-cause 30-day readmission rates but is associated with reduced 30-day readmission rates secondary to recurrent esophageal variceal bleeding. TIPS shows a modest survival advantage during index hospitalization when compared to EVB only.
Keywords: esophageal variceal banding; mortality; outcomes; readmission; recurrent esophageal variceal bleeding; tips.
Copyright © 2024, Shafiq et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Institutional Review Board of the University of Kansas Medical Center issued approval STUDY00161107. It has determined that the proposed activity is not a research involving human subjects as defined by DHHS and FDA regulations. The primary author of this study has a signed Healthcare Cost and Utilization Project (HCUP) data user agreement, which allowed access to the data used in this study. In HCUP data sets, 16 direct identifiers have been removed. For more information, please visit https://hcup-us.ahrq.gov/DUA/dua_508/DUA508version.jsp#hipaa and refer to the HIPAA section. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Competing risks and prognostic stages of cirrhosis: a 25-year inception cohort study of 494 patients. D'Amico G, Pasta L, Morabito A, et al. Aliment Pharmacol Ther. 2014;39:1180–1193. - PubMed
-
- A multicenter evaluation of adherence to 4 major elements of the baveno guidelines and outcomes for patients with acute variceal hemorrhage. Tapper EB, Friderici J, Borman ZA, et al. J Clin Gastroenterol. 2018;52:172–177. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials