

Evisceration and ocular prosthetic implantation following endovascular coiling for the management of endophthalmitis in a long-standing post-traumatic unilateral carotid-cavernous fistula: A case report and review of the literature
- PMID: 39651520
- PMCID: PMC11620303
- DOI: 10.4103/ojo.ojo_41_24
Evisceration and ocular prosthetic implantation following endovascular coiling for the management of endophthalmitis in a long-standing post-traumatic unilateral carotid-cavernous fistula: A case report and review of the literature
Abstract
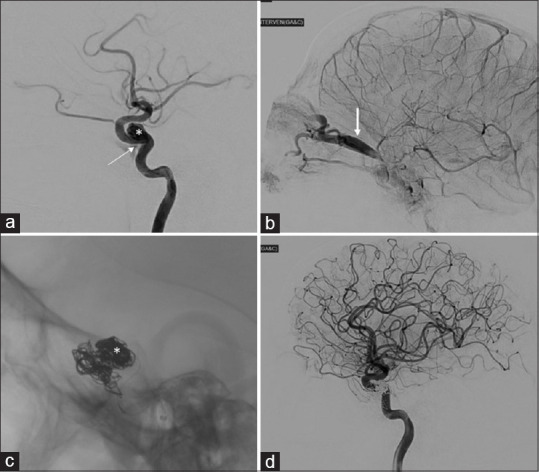
Carotid-cavernous fistula (CCF) is a rare condition involving an abnormal communication between the carotid artery and the cavernous sinus. We present a unique case of posttraumatic unilateral CCF initially misdiagnosed as a corneal melt with iris prolapse and orbital cellulitis. The patient, a 25-year-old male, experienced swelling, bleeding, and sudden vision loss in the affected eye following a fall. Imaging confirmed a direct CCF, and the patient underwent endovascular coiling, evisceration, and prosthetic replacement. Partial loss of levator palpebrae superioris muscle function was observed postprocedure. This case underscores the diagnostic challenge of CCF and highlights the significance of early and accurate diagnosis for appropriate management.
Keywords: Carotid-cavernous fistula; endovascular procedures; eye injuries; orbital cellulitis.
Copyright: © 2024 Oman Ophthalmic Society.
Conflict of interest statement
There are no conflicts of interest.
Figures


References
-
- Ellis JA, Goldstein H, Connolly ES, Jr, Meyers PM. Carotid-cavernous fistulas. Neurosurg Focus. 2012;32:E9. - PubMed
-
- Liang W, Xiaofeng Y, Weiguo L, Wusi Q, Gang S, Xuesheng Z. Traumatic carotid cavernous fistula accompanying basilar skull fracture: A study on the incidence of traumatic carotid cavernous fistula in the patients with basilar skull fracture and the prognostic analysis about traumatic carotid cavernous fistula. J Trauma. 2007;63:1014–20. - PubMed
-
- Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985;62:248–56. - PubMed
-
- Srinivas HV, Murthy S, Brown R. Is valsalva manoeuvre useful in diagnosing dural caroticocavernous fistulas? Eye (Lond) 2005;19:1226–7. - PubMed
-
- Adam CR, Shields CL, Gutman J, Kim HJ, Hayek B, Shore JW, et al. Dilated superior ophthalmic vein: Clinical and radiographic features of 113 cases. Ophthalmic Plast Reconstr Surg. 2018;34:68–73. - PubMed
Publication types
LinkOut - more resources
Full Text Sources