

Blinatumomab in Standard-Risk B-Cell Acute Lymphoblastic Leukemia in Children
- PMID: 39651791
- PMCID: PMC11864901
- DOI: 10.1056/NEJMoa2411680
Blinatumomab in Standard-Risk B-Cell Acute Lymphoblastic Leukemia in Children
Abstract
Background: B-cell acute lymphoblastic leukemia (B-cell ALL) is the most common childhood cancer. Despite a high overall cure rate, relapsed B-cell ALL remains a leading cause of cancer-related death among children. The addition of the bispecific T-cell engager molecule blinatumomab (an anti-CD19 and anti-CD3 single-chain molecule) to therapy for newly diagnosed standard-risk (as defined by the National Cancer Institute) B-cell ALL in children may improve outcomes.
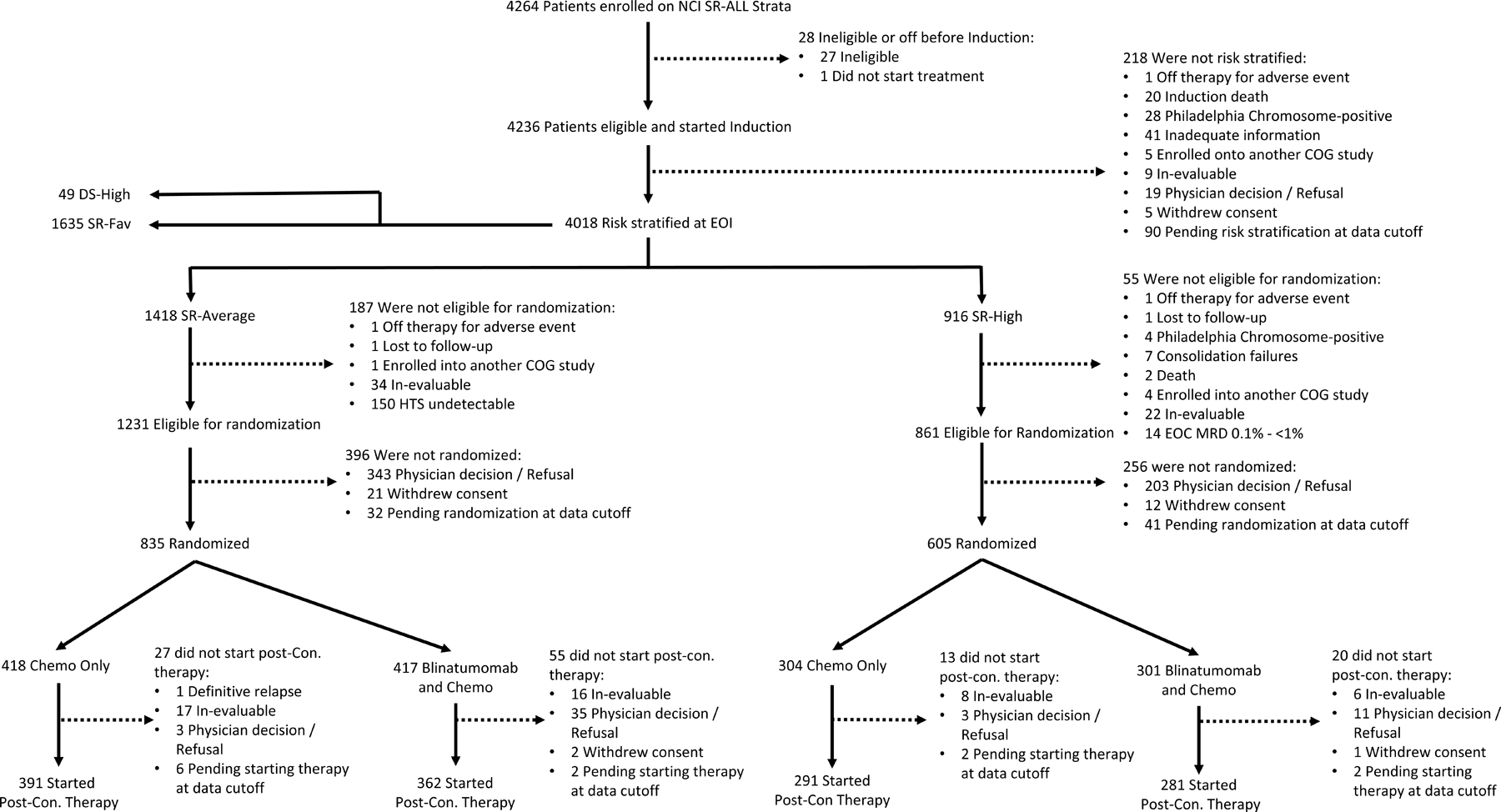
Methods: We conducted a phase 3 trial involving children with newly diagnosed standard-risk B-cell ALL who had an average or higher risk of relapse. Patients were randomly assigned to receive chemotherapy alone or chemotherapy plus two nonsequential 28-day cycles of blinatumomab. The primary end point was disease-free survival.
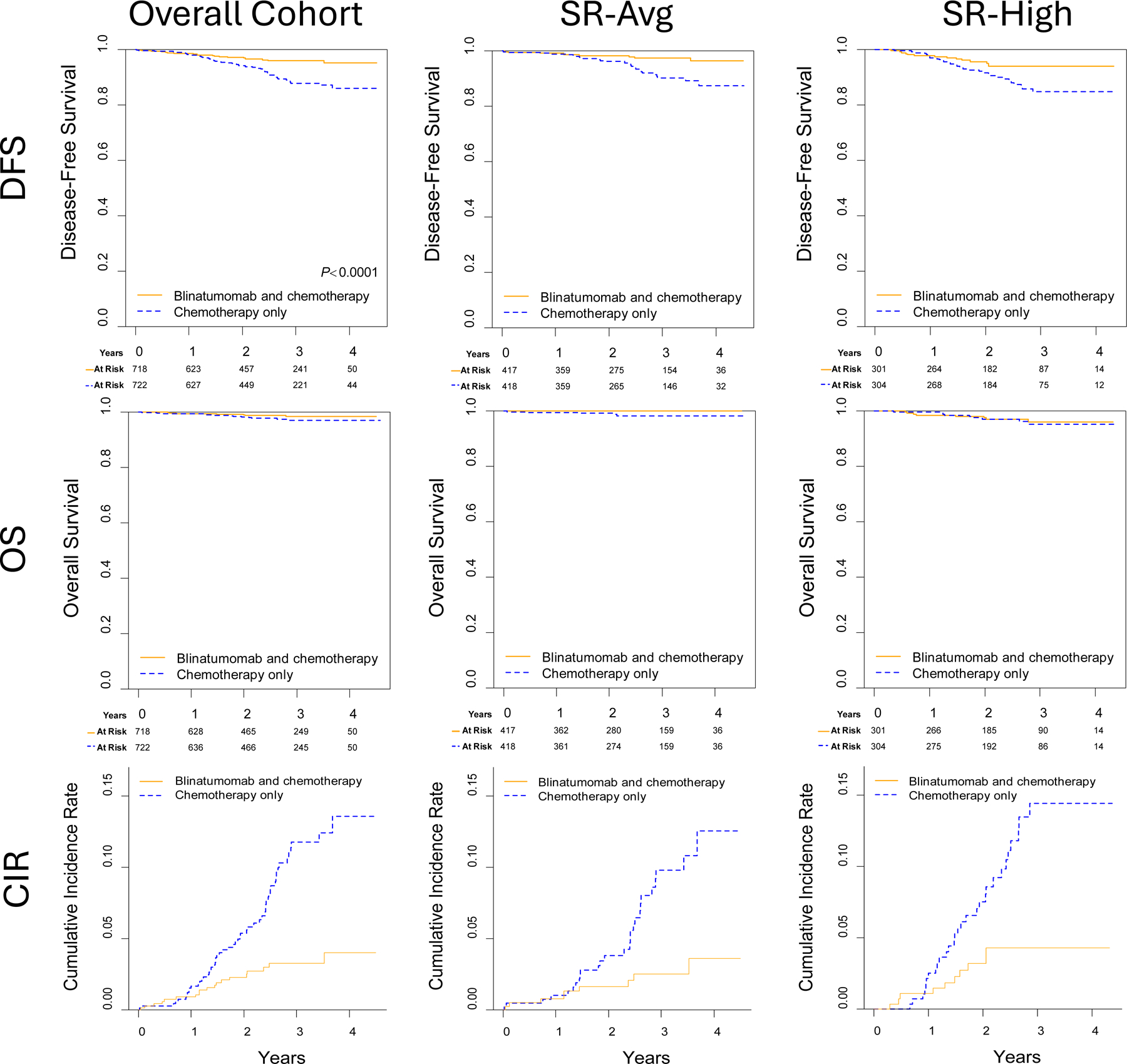
Results: The data and safety monitoring committee reviewed the results from the first interim efficacy analysis, which included 1440 patients who had undergone randomization (722 to chemotherapy alone and 718 to blinatumomab and chemotherapy) and recommended early termination of randomization. At a median follow-up of 2.5 years, the estimated 3-year disease-free survival (±SE) was 96.0±1.2% with blinatumomab and chemotherapy and 87.9±2.1% with chemotherapy alone (difference in restricted mean survival time, 72 days; 95% confidence interval, 36 to 108; P<0.001 by stratified log-rank test). The estimated 3-year disease-free survival among patients with an average relapse risk was 97.5±1.3% with blinatumomab and chemotherapy and 90.2±2.3% with chemotherapy alone; among those with a higher relapse risk, the corresponding values were 94.1±2.5% and 84.8±3.8%. Cytokine release syndrome, seizures, and sepsis of grade 3 or higher were rare during blinatumomab cycles, but the overall incidence of nonfatal sepsis and catheter-related infections was significantly higher among patients with an average relapse risk who had been assigned to receive blinatumomab and chemotherapy than among those assigned to receive chemotherapy alone.
Conclusions: Adding blinatumomab to combination chemotherapy in patients with newly diagnosed childhood standard-risk B-cell ALL of average or higher risk of relapse significantly improved disease-free survival. (Funded by the National Institutes of Health and others; AALL1731 ClinicalTrials.gov number, NCT03914625.).
Copyright © 2024 Massachusetts Medical Society.
Figures

Comment in
-
Blinatumomab in Childhood B-Cell Acute Lymphoblastic Leukemia.N Engl J Med. 2025 Jun 12;392(22):2286. doi: 10.1056/NEJMc2504183. N Engl J Med. 2025. PMID: 40499181 No abstract available.
-
Blinatumomab in Childhood B-Cell Acute Lymphoblastic Leukemia. Reply.N Engl J Med. 2025 Jun 12;392(22):2286-2287. doi: 10.1056/NEJMc2504183. N Engl J Med. 2025. PMID: 40499182 No abstract available.
References
-
- Hunger SP, Mullighan CG. Acute lymphoblastic leukemia in children. New Engl J Med 2015;373:1541–2. - PubMed
-
- Mattano LA, Devidas M, Friedmann AM, et al. Outstanding Outcome for Children with Standard Risk-Low (SR-Low) Acute Lymphoblastic Leukemia (ALL) and No Benefit to Intensified Peg-Asparaginase (PEG-ASNase) Therapy: Results of Children’s Oncology Group (COG) Study AALL0331. Blood 2014;124:Abstract 793.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical