

The Effect of Cranial Sutures Should Be Considered in Transcranial Electrical Stimulation
- PMID: 39652012
- PMCID: PMC12105966
- DOI: 10.1097/YCT.0000000000001079
The Effect of Cranial Sutures Should Be Considered in Transcranial Electrical Stimulation
Abstract
Background: Computational modeling is used to optimize transcranial electrical stimulation (tES) approaches, and the precision of these models is dependent on their anatomical accuracy. We are unaware of any computational modeling of tES that has included cranial sutures.
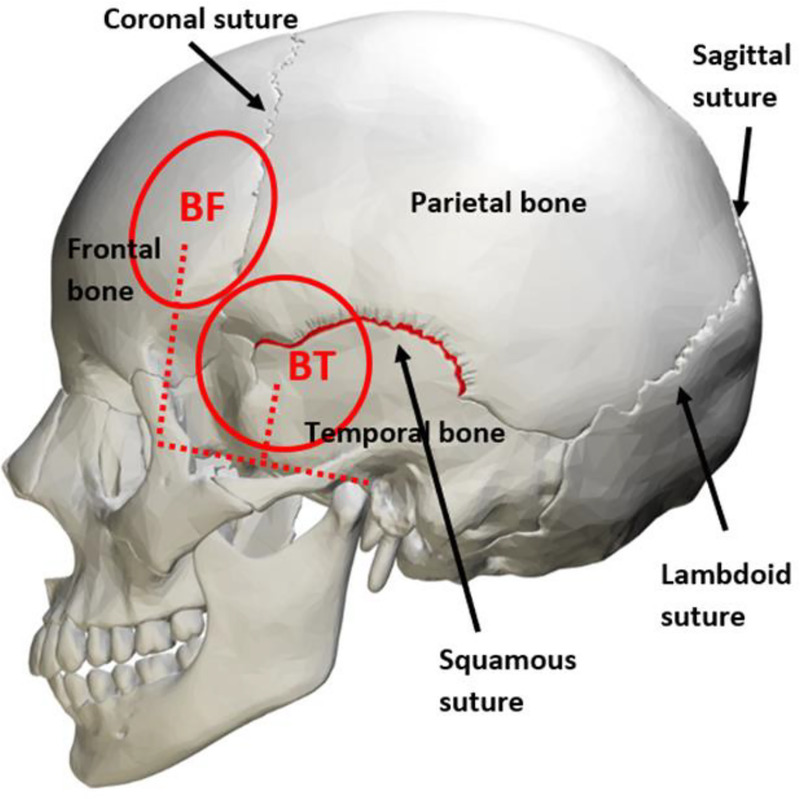
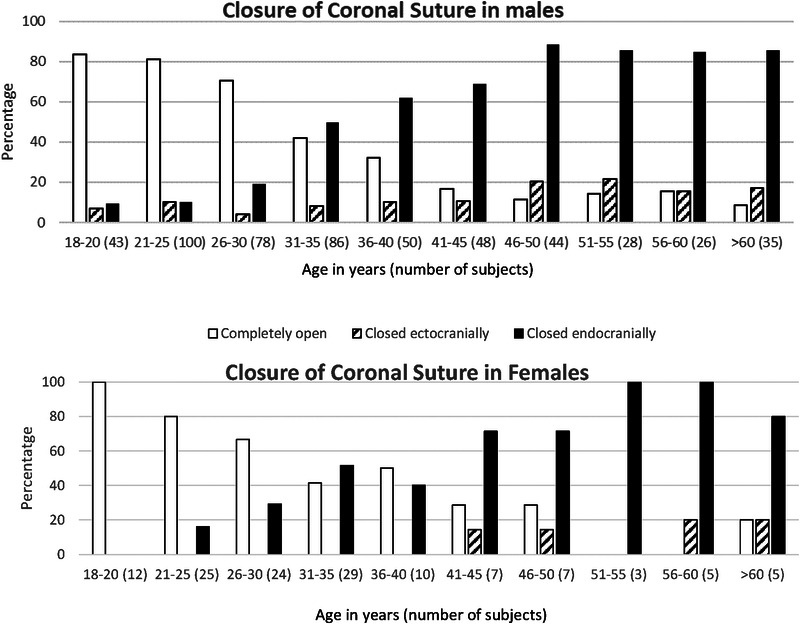
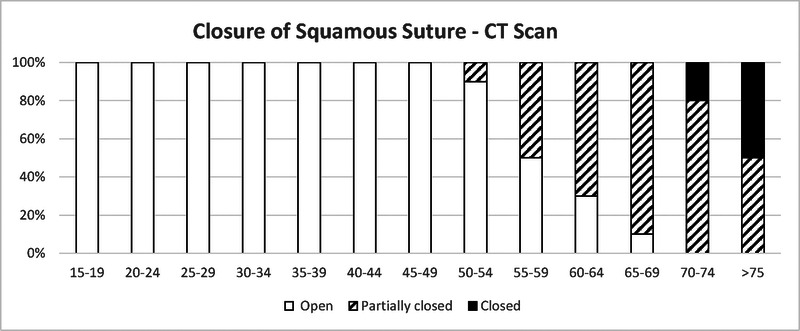
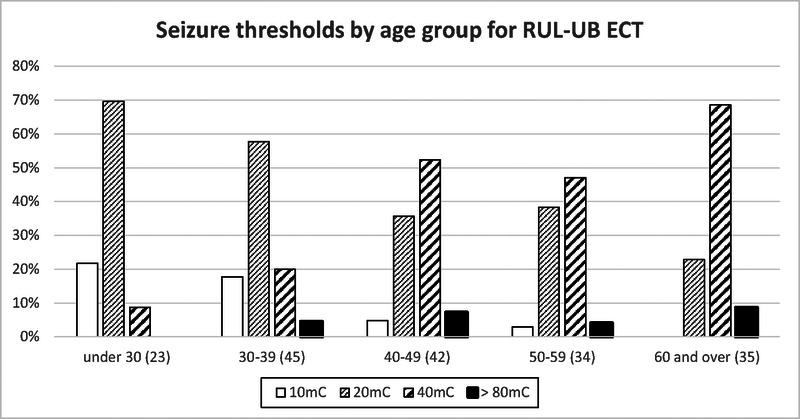
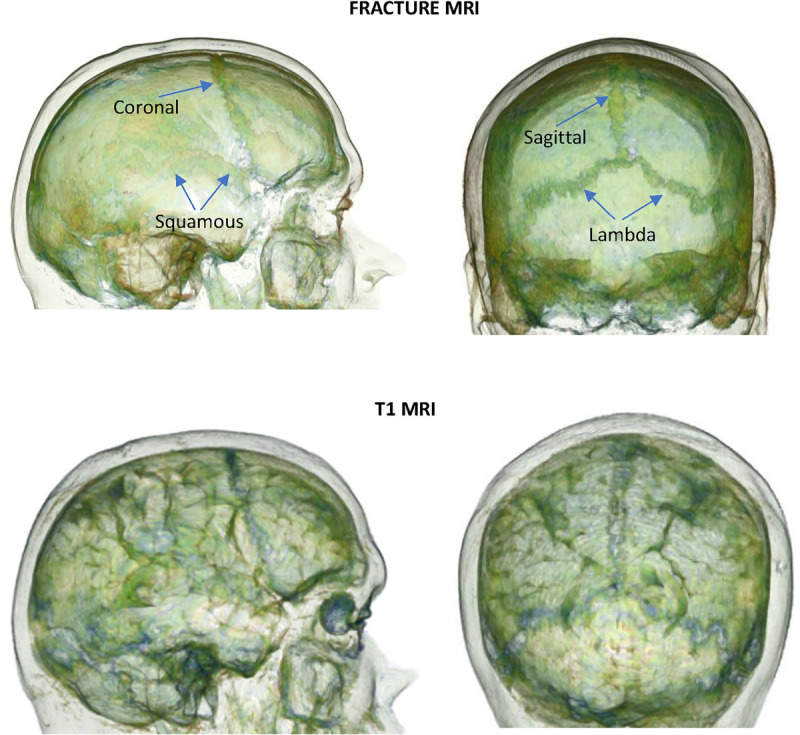
Objectives: The aims of the study were to review the literature on the timing of closure of the coronal and squamous sutures, which are situated under electrode placements used in tES; to review the literature regarding differences in skull and suture conductivity and to determine a more accurate conductivity for sutures; and to identify magnetic resonance image (MRI) techniques that could be used to detect cranial sutures.
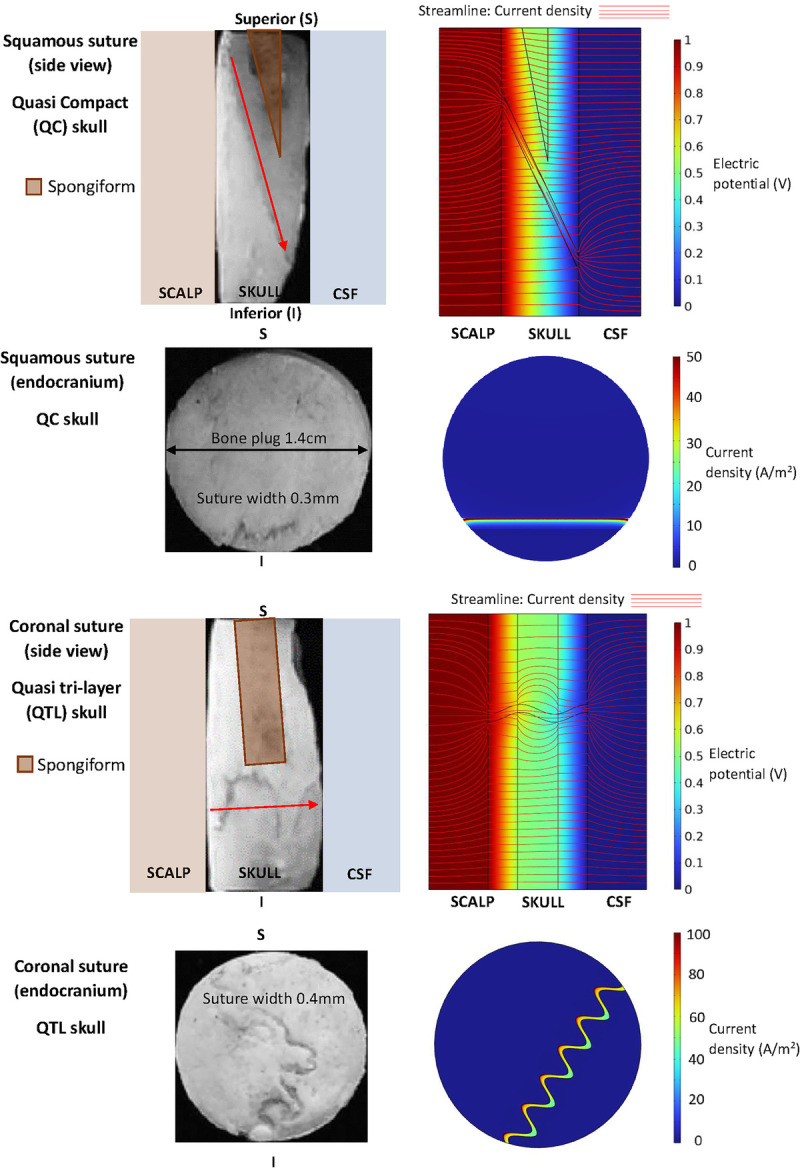
Methods: A scoping review of medical literature was conducted. We conducted computational modeling of a cranial bone plug using COMSOL Multiphysics finite element software, utilizing methodology and results from a previous study. We assessed use of the "3D Slicer" software to identify sutures in routine T1-weighted MRI scans.
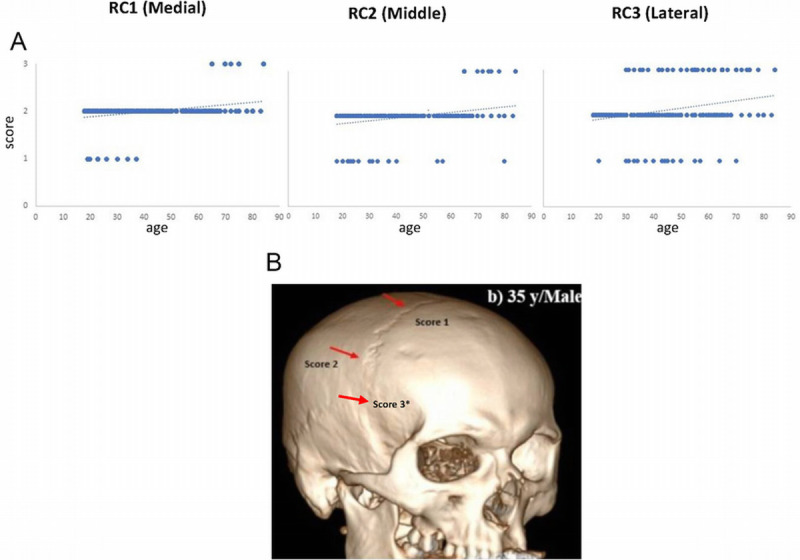
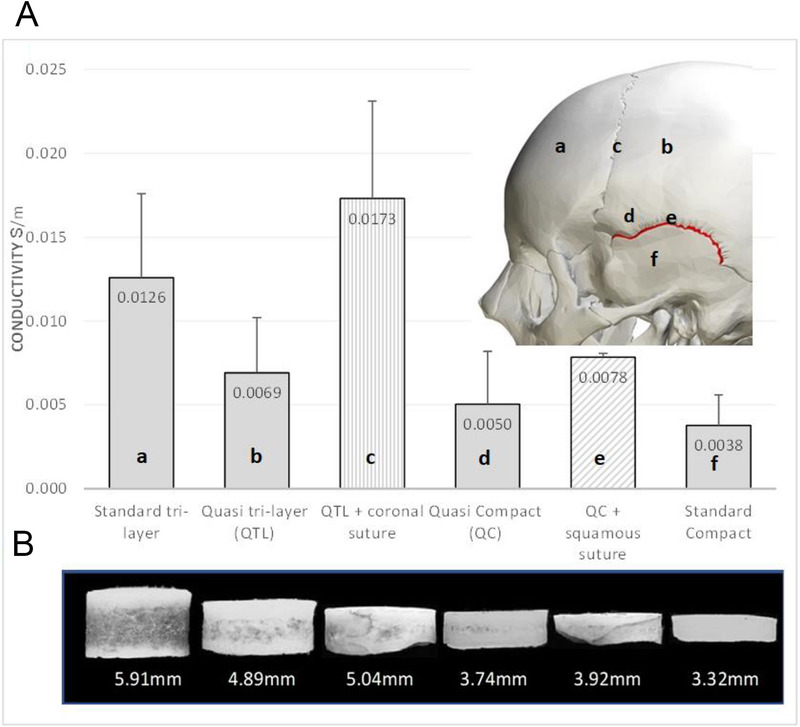
Results: Reports from forensic examinations and computed tomography (CT) scans showed suture closure does not correlate with age. Our computational modeling determined a cranial suture conductivity of 0.32 S/m, which is much higher than for skull (compact skull 0.004 S/m, standard trilayer 0.013 S/m). 3D slicer enabled rapid and precise identification of the anatomy and location of cranial sutures.
Conclusions: Cranial sutures persist throughout the lifespan and have a far higher conductivity than skull bone. Cranial sutures can be localized quickly and precisely using a combination of MRI and readily available modeling software. Sutures should be included in tES computational modeling and electroencephalography source imaging to improve the accuracy of results.
Keywords: EEG; computational modeling; cranial suture conductance; transcranial electrical stimulation.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest or financial disclosures to report.
Figures
Similar articles
-
Cranial Sutures Alter Computational Models of Transcranial Electrical Stimulation.J ECT. 2025 May 2. doi: 10.1097/YCT.0000000000001154. Online ahead of print. J ECT. 2025. PMID: 40341556
-
Enhanced tES and tDCS computational models by meninges emulation.J Neural Eng. 2020 Jan 14;17(1):016027. doi: 10.1088/1741-2552/ab549d. J Neural Eng. 2020. PMID: 31689695 Free PMC article.
-
Microfocal CT: a method for evaluating murine cranial sutures in situ.J Surg Res. 2004 Feb;116(2):322-9. doi: 10.1016/j.jss.2003.10.001. J Surg Res. 2004. PMID: 15013372
-
Occipital sutures and its variations: the value of 3D-CT and how to differentiate it from fractures using 3D-CT?Surg Radiol Anat. 2010 Nov;32(9):807-16. doi: 10.1007/s00276-010-0633-5. Epub 2010 Feb 23. Surg Radiol Anat. 2010. PMID: 20174986 Review.
-
CT of Normal Developmental and Variant Anatomy of the Pediatric Skull: Distinguishing Trauma from Normality.Radiographics. 2015 Sep-Oct;35(5):1585-601. doi: 10.1148/rg.2015140177. Epub 2015 Jul 24. Radiographics. 2015. PMID: 26207580 Review.
References
-
- UK ECT Review Group . Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis. Lancet. 2003;361:799–808. - PubMed
-
- Lefaucheur JP Antal A Ayache SS, et al. . Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin Neurophysiol. 2017;128:56–92. - PubMed
-
- Alam M, et al. . A study on differences in the obliteration of cranial sutures and their clinical significance. J Anat Soc India. 2020;69:97–102.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
