

Artificial intelligence after the bedside: co-design of AI-based clinical informatics workflows to routinely analyse patient-reported experience measures in hospitals
- PMID: 39653514
- PMCID: PMC11628959
- DOI: 10.1136/bmjhci-2024-101124
Artificial intelligence after the bedside: co-design of AI-based clinical informatics workflows to routinely analyse patient-reported experience measures in hospitals
Abstract
Objective: To co-design artificial intelligence (AI)-based clinical informatics workflows to routinely analyse patient-reported experience measures (PREMs) in hospitals.
Methods: The context was public hospitals (n=114) and health services (n=16) in a large state in Australia serving a population of ~5 million. We conducted a participatory action research study with multidisciplinary healthcare professionals, managers, data analysts, consumer representatives and industry professionals (n=16) across three phases: (1) defining the problem, (2) current workflow and co-designing a future workflow and (3) developing proof-of-concept AI-based workflows. Co-designed workflows were deductively mapped to a validated feasibility framework to inform future clinical piloting. Qualitative data underwent inductive thematic analysis.
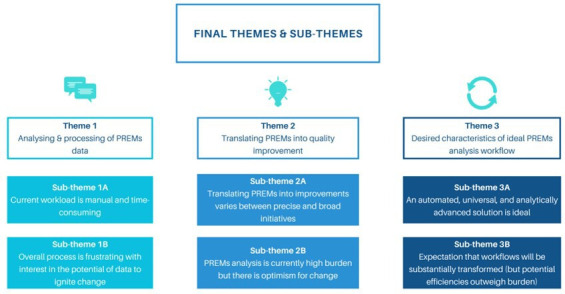
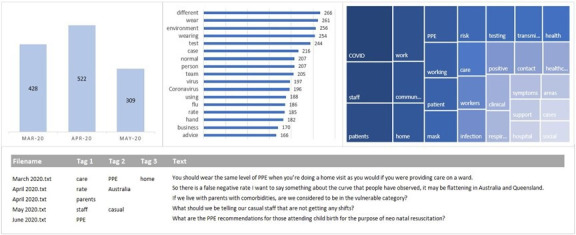
Results: Between 2020 and 2022 (n=16 health services), 175 282 PREMs inpatient surveys received 23 982 open-ended responses (mean response rate, 13.7%). Existing PREMs workflows were problematic due to overwhelming data volume, analytical limitations, poor integration with health service workflows and inequitable resource distribution. Three potential semiautomated, AI-based (unsupervised machine learning) workflows were developed to address the identified problems: (1) no code (simple reports, no analytics), (2) low code (PowerBI dashboard, descriptive analytics) and (3) high code (Power BI dashboard, descriptive analytics, clinical unit-level interactive reporting).
Discussion: The manual analysis of free-text PREMs data is laborious and difficult at scale. Automating analysis with AI could sharpen the focus on consumer input and accelerate quality improvement cycles in hospitals. Future research should investigate how AI-based workflows impact healthcare quality and safety.
Conclusion: AI-based clinical informatics workflows to routinely analyse free-text PREMs data were co-designed with multidisciplinary end-users and are ready for clinical piloting.
Keywords: Health Services Research; Machine Learning; Medical Informatics; Patient-Centered Care.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: Funding for this research was provided by Queensland Health as the state hospital and health service in Queensland, Australia, and administered to the Queensland Digital Health Centre, Faculty of Medicine, The University of Queensland via a Professional Services Agreement (no grant/award number). Queensland Health had no role in conducting, analysing or reporting the research. Philips Electronics Australia Limited is contracted by Queensland Health to provide Questionnaire Manager, the electronic system that collects patient-reported experience measures. As Program Manager of the Queensland Health Patient Reported Experience and Outcome Measures program, JD has a professional relationship with stakeholders involved in key informant interviews. There is no past or present commercial or financial relationship with Leximancer, and Leximancer had no role in conducting, analysing, or reporting the research.
Figures
Similar articles
-
Artificial intelligence for breast cancer detection and its health technology assessment: A scoping review.Comput Biol Med. 2025 Jan;184:109391. doi: 10.1016/j.compbiomed.2024.109391. Epub 2024 Nov 22. Comput Biol Med. 2025. PMID: 39579663
-
Partnering with consumers to co-design a person-centred coding framework for qualitative patient experience data.Patient Educ Couns. 2023 Nov;116:107938. doi: 10.1016/j.pec.2023.107938. Epub 2023 Aug 12. Patient Educ Couns. 2023. PMID: 37598583
-
Clinician Perceptions of Generative Artificial Intelligence Tools and Clinical Workflows: Potential Uses, Motivations for Adoption, and Sentiments on Impact.AMIA Annu Symp Proc. 2025 May 22;2024:960-969. eCollection 2024. AMIA Annu Symp Proc. 2025. PMID: 40417507 Free PMC article.
-
What is measured matters: A scoping review of analysis methods used for qualitative patient reported experience measure data.Int J Med Inform. 2024 Oct;190:105559. doi: 10.1016/j.ijmedinf.2024.105559. Epub 2024 Jul 18. Int J Med Inform. 2024. PMID: 39032453
-
Understanding the factors influencing acceptability of AI in medical imaging domains among healthcare professionals: A scoping review.Artif Intell Med. 2024 Jan;147:102698. doi: 10.1016/j.artmed.2023.102698. Epub 2023 Nov 9. Artif Intell Med. 2024. PMID: 38184343
References
MeSH terms
LinkOut - more resources
Full Text Sources