

Comparison of different treatment options in submacular haemorrhage
- PMID: 39654042
- PMCID: PMC11626755
- DOI: 10.1186/s12886-024-03794-y
Comparison of different treatment options in submacular haemorrhage
Abstract
Background/aims: Submacular haemorrhages (SMH) cause significant visual impairment. Until now, the comparative effectiveness of different treatment approaches remains inconclusive without clear treatment guidelines. The aim of our study was to evaluate the effectiveness of 5 surgical treatment modalities in terms of visual prognosis and success rate.
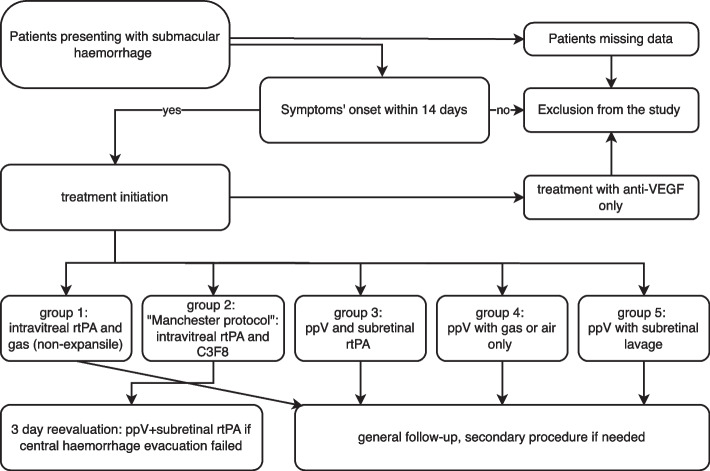
Methods: This retrospective study included 201 patients with SMH. Primary endpoint was best corrected visual acuity (BCVA), secondary endpoints included haemorrhage size and complications. Group 1 was treated with pneumatic displacement and rtPA-injection. Group 2 followed the "Manchester protocol" with rtPA-injection and-if needed-a standardised secondary procedure with pars plana vitrectomy (ppV) and subretinal rtPA. Group 3 underwent vitrectomy with subretinal rtPA, group 4 vitrectomy only and group 5 received subretinal lavage.
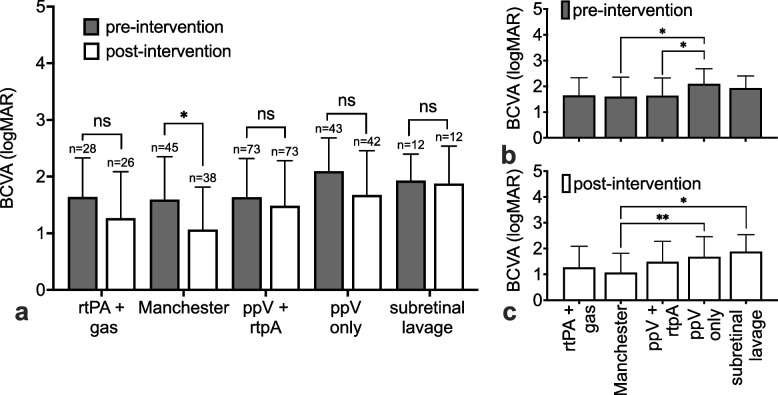
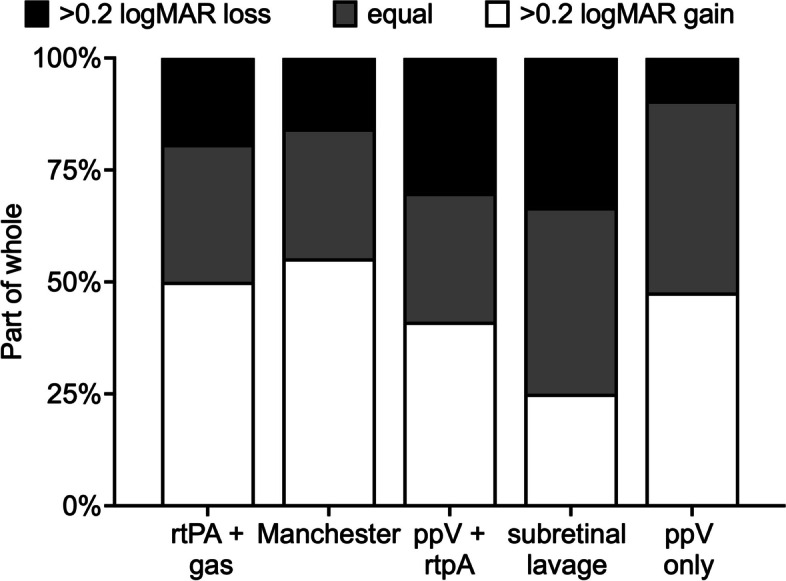
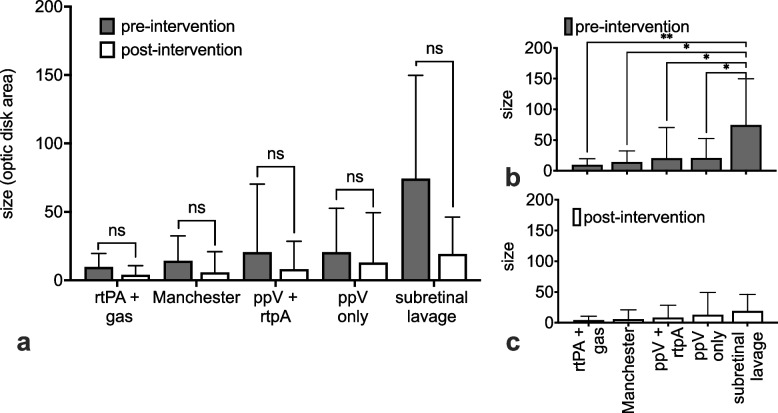
Results: Baseline characteristics were a mean age of 79 years and a follow-up of 4.6 months. Pre-intervention BCVA of 1.7 logMAR improved to 1.4 logMAR at follow-up. A gain of > 0.2 logMAR was achieved in 47% of patients, while 20% lost > 0.2 logMAR. Only group 2 achieved a statistically significant visual gain. While group 5 was statistically larger in haemorrhage size preoperatively (p < 0.05), all groups were statistically equal in SMH size at follow-up. Complications led to additional interventions in 20% of patients.
Conclusions: No significant change in visual prognosis could be achieved depending on the intervention. As more invasive techniques seem to lack the benefit of a better postoperative prognosis while carrying higher risks, it may be beneficial considering a less invasive option first.
Keywords: Macular degeneration; Macular haemorrhage; Pars plana vitrectomy; Pneumatic displacement; Recombinant Plasminogen activator; RtPA; Submacular haemorrhage; Subretinal haemorrhage; Subretinal lavage.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee from the university of Ulm (460/22, Date: 19.12.2022). Informed consent to participate was obtained from all participants. The authors confirm that the ethical policies of the journal have been adhered to and the appropriate ethical review committee approval has been received. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Toth CA, Morse LS, Hjelmeland LM, Landers MB 3rd. Fibrin directs early retinal damage after experimental subretinal hemorrhage. Arch Ophthalmol. 1991;109(5):723–9. - PubMed
-
- Coll GE, Sparrow JR, Marinovic A, Chang S. Effect of intravitreal tissue plasminogen activator on experimental subretinal hemorrhage. Retina. 1995;15(4):319–26. - PubMed
-
- Scupola A, Coscas G, Soubrane G, Balestrazzi E. Natural history of macular subretinal hemorrhage in age-related macular degeneration. Ophthalmologica. 1999;213(2):97–102. - PubMed
-
- Glatt H, Machemer R. Experimental Subretinal Hemorrhage in Rabbits. Am J Ophthalmol. 1982;94(6):762–73. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
