

Neutrophils extracellular traps myeloperoxidase and elastase predict cerebral vasospasms after aneurysmal subarachnoid hemorrhage
- PMID: 39654759
- PMCID: PMC11625263
- DOI: 10.1016/j.heliyon.2024.e40562
Neutrophils extracellular traps myeloperoxidase and elastase predict cerebral vasospasms after aneurysmal subarachnoid hemorrhage
Abstract
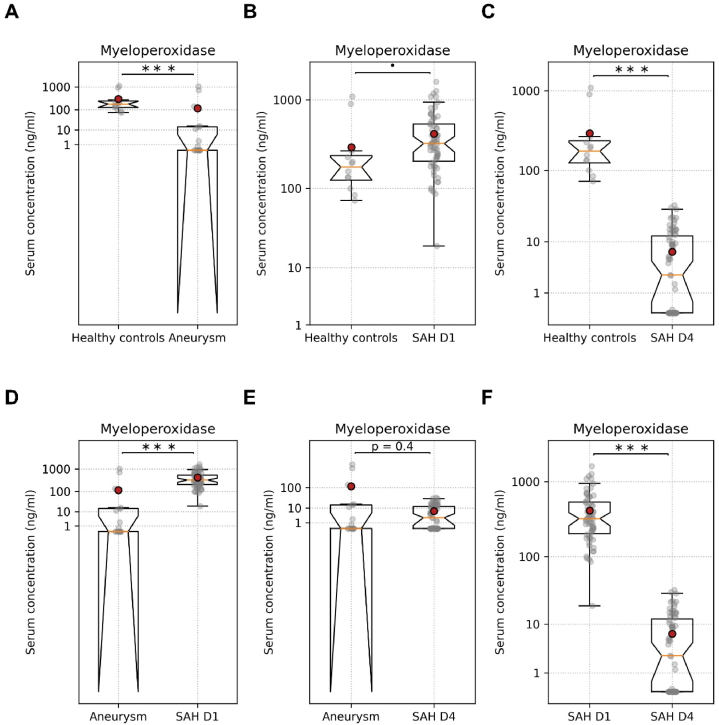
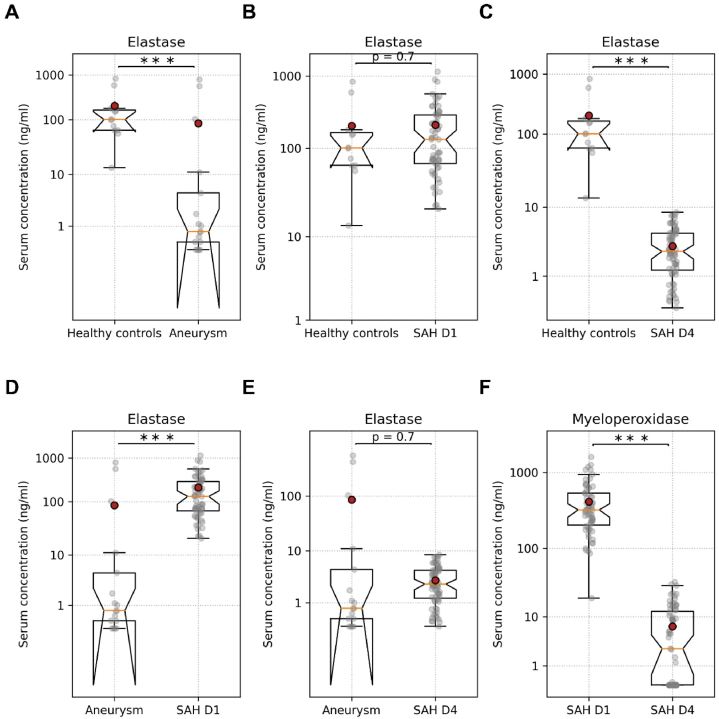
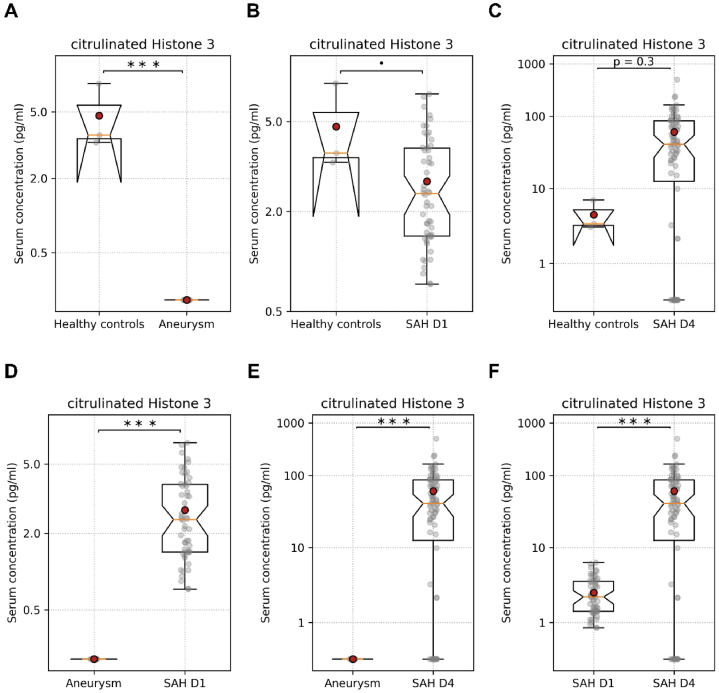
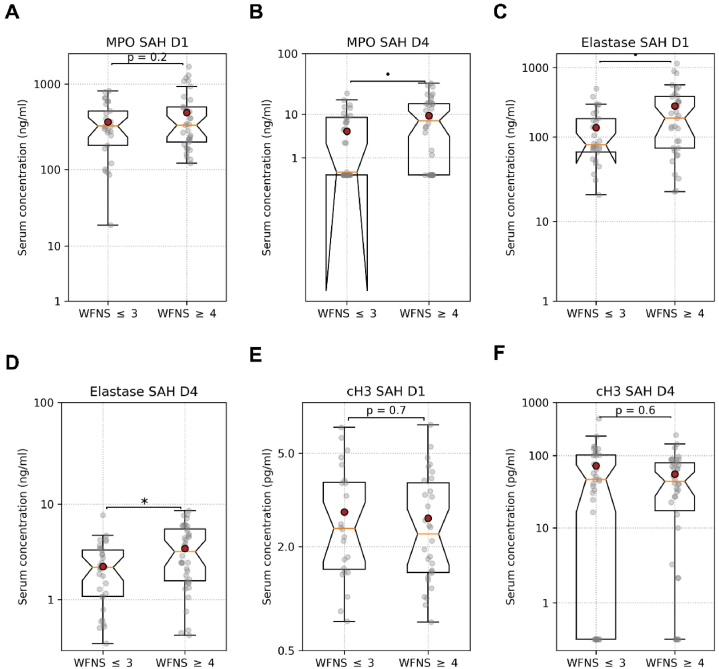
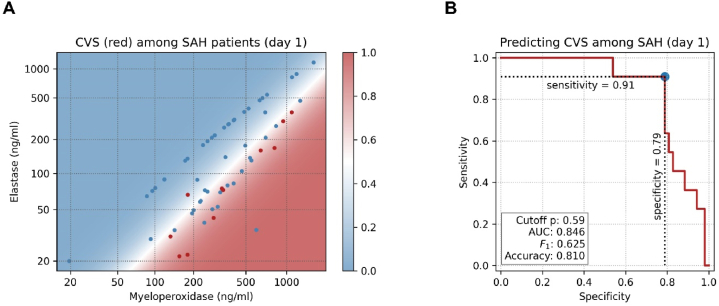
Aneurysmal subarachnoid hemorrhage (aSAH) is a highly fatal and morbid disease. Despite successful coiling or clipping of a ruptured aneurysm, the patients suffer post-aSAH complications, including early brain injury, cerebral vasospasm (CVS), delayed cerebral ischemia (DCI), and systemic infections that mainly determine the clinical outcomes. Diagnostic biomarkers to predict accurately post-aSAH complications are needed. In this prospective exploratory study, we investigated the predictive value of neutrophil extracellular traps (NETs) components for CVS after aSAH. In the study, 62 patients with aSAH, 17 patients with unruptured cerebral aneurysms, and 12 healthy controls were included. The serum levels of myeloperoxidase (MPO), elastase (ELA), and citrullinated histone H3 (cH3) on day 1 and day 4 of hospital admission were measured with ELISA. Data were scaled using the Yeo-Johnson transformation. Values in two groups were compared using a t-test and in multiple groups using ANOVA. Logistic regression was used to model the outcome probability, including CVS, as the function of ELISA values. Among the patients with aneurysms, those who suffered aSAH had significantly higher levels of MPO (113.9 ± 294.4 vs. 422.3 ± 319.0 ng/ml, p < 0.05), ELA (84.8 ± 221.0 vs. 199.2 ± 218.9 ng/ml, p < 0.05), and cH3 (0.0 ± 0.0 vs. 2.8 ± 1.5, ng/ml, p < 0.05) on day one after aSAH, suggesting the involvement of NETs components in pathophysiology of aSAH and the events following aSAH. Individually, MPO and ELA levels taken on day 1 after SAH did not differ between patients with CVS and patients without CVS. However, when taken together into a logistic model, they allowed for predicting CVS with high sensitivity (91 %) and specificity (79 %). MPO and ELA, along with other clinical parameters, can be used as early predictors of CVS in aSAH patients and can serve as guidance during treatment decisions in the management of aSAH.
Keywords: Cerebral vasospasm; Elastase; Myeloperoxidase; Predictive model; aSAH.
© 2024 The Authors. Published by Elsevier Ltd.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Neutrophil Extracellular Traps and Delayed Cerebral Ischemia in Aneurysmal Subarachnoid Hemorrhage.Crit Care Explor. 2022 May 17;4(5):e0692. doi: 10.1097/CCE.0000000000000692. eCollection 2022 May. Crit Care Explor. 2022. PMID: 35620772 Free PMC article.
-
CLR (C-Reactive Protein to Lymphocyte Ratio) Served as a Promising Predictive Biomarker for Cerebral Vasospasm in Aneurysmal Subarachnoid Hemorrhage (aSAH): A Retrospective Cohort Study.J Clin Med. 2024 Feb 6;13(4):940. doi: 10.3390/jcm13040940. J Clin Med. 2024. PMID: 38398254 Free PMC article.
-
Elevated Systemic IL-6 Levels in Patients with Aneurysmal Subarachnoid Hemorrhage Is an Unspecific Marker for Post-SAH Complications.Int J Mol Sci. 2017 Dec 1;18(12):2580. doi: 10.3390/ijms18122580. Int J Mol Sci. 2017. PMID: 29194369 Free PMC article.
-
Electroencephalography for detection of vasospasm and delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage: a retrospective analysis and systematic review.Neurosurg Focus. 2022 Mar;52(3):E3. doi: 10.3171/2021.12.FOCUS21656. Neurosurg Focus. 2022. PMID: 35231893
-
Targeting High Mobility Group Box 1 in Subarachnoid Hemorrhage: A Systematic Review.Int J Mol Sci. 2020 Apr 14;21(8):2709. doi: 10.3390/ijms21082709. Int J Mol Sci. 2020. PMID: 32295146 Free PMC article.
Cited by
-
Development of an enzyme-linked immunosorbent assay (ELISA) for determining neutrophil elastase (NE) - a potential useful marker of multi-organ damage observed in COVID-19 and post-Covid-19 (PCS).Front Mol Biosci. 2025 Feb 25;12:1542898. doi: 10.3389/fmolb.2025.1542898. eCollection 2025. Front Mol Biosci. 2025. PMID: 40070691 Free PMC article.
References
-
- Hackenberg K.A.M., Hanggi D., Etminan N. Unruptured intracranial aneurysms. Stroke. 2018;49(9):2268–2275. - PubMed
-
- Rehman S., et al. Case-fatality and functional outcome after subarachnoid hemorrhage (SAH) in INternational STRoke oUtComes sTudy (INSTRUCT) J. Stroke Cerebrovasc. Dis. 2022;31(1) - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
