

Racial and regional disparities in the risk of noncommunicable disease between sub-Saharan black and European white patients
- PMID: 39655600
- PMCID: PMC11789602
- DOI: 10.1097/HJH.0000000000003930
Racial and regional disparities in the risk of noncommunicable disease between sub-Saharan black and European white patients
Abstract
Objectives: Greater vulnerability of Black vs. White individuals to cardiovascular disease (CVD) and chronic kidney disease (CKD) is well charted in the United States, but studies involving sub-Saharan blacks are scarce.
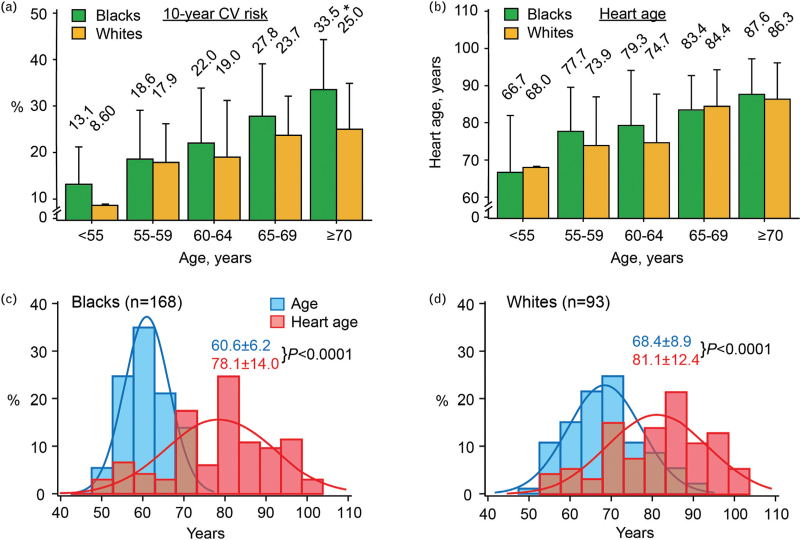
Methods: Baseline data (2021-2024) were collected in 168 sub-Saharan Blacks and 93 European Whites in an ongoing clinical trial (NCT04299529), using standardized patient selection criteria. Data included clinical and biochemical risk factors, ECG and echocardiographic traits, Framingham CVD risk, CKD grades (KDIGO 2024), self-assessed symptoms (WHO questionnaire), and urinary proteomic profiles predictive of left ventricular dysfunction (LVD) and CKD, HF1, and CKD273, respectively. Racial comparisons rested on unadjusted and multivariable-adjusted analyses.
Results: Despite being younger (60.4 vs. 68.3 years), blacks had a worse risk profile, as evidenced by higher diabetes prevalence, higher BMI, faster heart rate, unfavourable serum cholesterol fractions, lower estimated glomerular filtration rate, microalbuminuria, and sedentary lifestyle. This resulted in blacks having higher 10-year CVD risk, higher heart age (index of vascular ageing with chronological age as reference), and a worse CKD grades. In both races, CKD273 increased with CKD grade, but CKD273 and HF1 were not different by race. These observations were robust in subgroup and adjusted analyses.
Conclusion: This study did not differentiate host (genetic, molecular, and pathogenic) from environmental drivers of disease. Nonetheless, the findings call for a multipronged and comprehensive implementation of innovative health policies in sub-Saharan countries. Education, research, empowerment of stakeholders, and international learned societies connecting experts from a wide array of disciplines should vigorously sustain this effort.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Harald Mischak is the founder and co-owner of Mosaiques Diagnostics (Hannover, Germany). Agnieszka Latosinska is employed by Mosaiques Diagnostics. The other co-authors declare no conflict of interest.
Figures



References
-
- Agyepong IA, Sewanjamba N, Binawaho A, Coll-Seck AM, Carrah T, Ezeh A, et al. . The path to longer and healthier lives for all Africans by 2030: the Lancet Commission on future health in sub-Saharan Africa. Lancet 2017; 390:2803–2859. - PubMed
-
- Keates AK, Mocumbi AO, Ntsekhe M, Sliwa K, Stewart S. Cardiovascular disease in Africa: epidemiological profile and challenges. Nat Rev Cardiol 2017; 14:273–293. - PubMed
-
- Schutte AE, Botha S, Fourie CMT, Gafane-Matemane LF, Kruger R, Lammertyn L, et al. . Recent advances in understanding hypertension development in sub-Saharan Africa. J Hum Hypertens 2017; 31:491–500. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
