

Post-discharge changes in nutritional status predict prognosis in patients with acute decompensated HFpEF from the PURSUIT-HFpEF Registry
- PMID: 39656282
- PMCID: PMC12165886
- DOI: 10.1007/s00380-024-02499-y
Post-discharge changes in nutritional status predict prognosis in patients with acute decompensated HFpEF from the PURSUIT-HFpEF Registry
Abstract
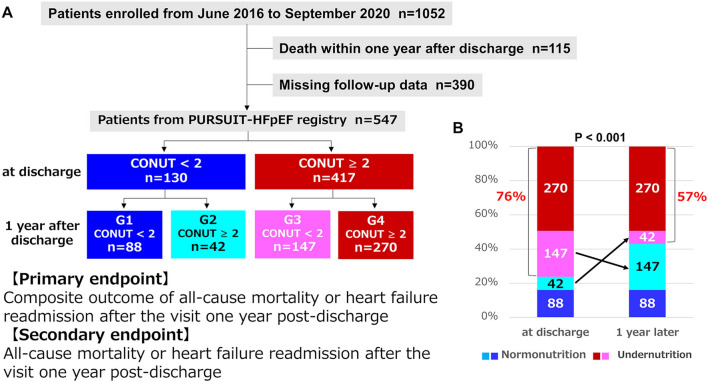
Undernutrition has been identified as a poor prognostic factor in heart failure with preserved ejection fraction (HFpEF). This study aimed to evaluate the impact of changes in nutritional status from discharge to one year post-discharge on the prognosis of patients with HFpEF. Initially, 547 HFpEF cases were classified into a normal nutrition group (NN) (n = 130) and an undernutrition group (UN) (n = 417), according to Controlling Nutritional Status (CONUT) scores at discharge. These groups were further subdivided according to CONUT scores one year post-discharge into NN (G1, n = 88) and UN (G2, n = 42), and NN (G3, n = 147) and UN (G4, n = 270), respectively. The primary end point was defined as a composite of all-cause mortality or heart failure readmission after the visit one year post-discharge. Normal nutrition was defined as a CONUT score of 0 or 1, and undernutrition as a CONUT score of ≥ 2. We compared the incidence rates of the primary end point between G1 and G2, and G3 and G4, and identified predictors for abnormalization or normalization of CONUT score one year post-discharge, as well as covarying factors with change in CONUT. In a multivariable Cox proportional hazards model, abnormalization of CONUT score was associated with an increased risk of the primary end point (adjusted HR [hazard ratio]: 2.87, 95% CI [confidence interval]: 1.32-6.22, p = 0.008), while normalization of CONUT was associated with a reduced risk (adjusted HR: 0.40, 95% CI: 0.23-0.67, p < 0.001). In a multivariate logistic regression analysis of patients with normal nutrition at discharge, the Euro Qol 5 Dimension score was identified as an independent predictor for abnormalization of CONUT score one year post-discharge (OR: 0.06, 95% CI: 0.01-0.43, p = 0.023). Among patients with undernutrition at discharge, prior heart failure hospitalization was the independent predictor for normalization of CONUT score (OR: 0.36, 95% CI: 0.20-0.66, p < 0.001). In a multivariate linear regression analysis, independent covariates associated with changes in CONUT included hemoglobin (β = - 0.297, p < 0.001), C-reactive protein (β = 0.349, p < 0.001), and log NT-proBNP (β = 0.142, p < 0.001). Post-discharge abnormalization or normalization of CONUT scores has prognostic impact on patients with HFpEF. Changes in CONUT may independently correlate with changes in hematopoiesis, inflammation, and fluid retention.
Keywords: Changes in nutritional status; Controlling nutritional status; Heart failure with preserved ejection fraction; Prognosis.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: Shungo Hikoso has received remuneration from Daiichi Sankyo Company, Boehringer Ingelheim Japan, AstraZeneca K.K. and Bayer, and research funding from Roche Diagnostics, FUJIFILM Toyama Chemical and Bristol Myers Squibb. Hiroya Mizuno has received a department endowment from Terumo. Yohei Sotomi has received remuneration from Abbott Vascular Japan, Boston Scientific Japan, research funding from Abbott Vascular Japan, and a department endowment from Terumo. Yasushi Sakata has received remuneration from Otsuka Pharmaceutical, Ono Pharmaceutical, Daiichi Sankyo Company and AstraZeneca K.K., and research funding from Otsuka Pharmaceutical, Daiichi Sankyo Company, Mitsubishi Tanabe Pharma Corporation, Astellas Pharma, Kowa Company, Boehringer Ingelheim Japan, and Biotronik. The other authors (Akihiro Sunaga, Shunsuke Tamaki, Masahiro Seo, Masamichi Yano, Takaharu Hayashi, Akito Nakagawa, Yusuke Nakagawa, Hiroyuki Kurakami, Tomomi Yamada, Tetsuhisa Kitamura, Taiki Sato, Bolrathanak Oeun, Hirota Kida, Tomoharu Dohi, Katsuki Okada, Daisaku Nakatani, Takahisa Yamada, Yoshio Yasumura) have no conflicts of interest to report. Ethical approval: IRB information—Kansai Rosai Hospital Institutional Review Board (approval ID: 16co10g), Kawachi General Hospital Ethics Committee (approval ID unavailable, but approved on 26 Apr 2016), Osaka Rosai Hospital Ethics Committee (approval ID: 28-5), Higashiosaka City Medical Center Institutional Review Board (approval ID: 02-0313), Osaka Prefectural Hospital Organization Osaka General Medical Center Institutional Review Board (approval ID: 28-2002), Hyogo Prefectural Nishinomiya Hospital Ethics Committee (approval ID: H28-3), Ikeda Municipal Hospital Ethics Committee (approval ID: 3280), Kawanishi City Hospital Institutional Review Board (approval ID: 28001), Rinku General Medical Center Ethics Committee (approval ID: 27-40), Saiseikai Senri Hospital Ethics Committee (approval ID: 280304), Yao Municipal Hospital Institutional Review Board (approval ID: H28-6), Kawasaki Hospital Ethics Committee (approval ID unavail able, but approved on 12 May 2016), Minoh City Hospital Ethics Committee (approval ID unavailable, but approved on 24 May 2016), National Hospital Organization Osaka National Hospital Second Institutional Review Board (approval ID: 16024), Kano General Hospital Ethics Committee (approval ID unavailable, but approved on 9 June 2016), Toyonaka Municipal Hospital Ethics Committee (approval ID: 2016-04-02), Kinan Hospital Ethics Committee 121, Japan Community Health Care Organization Osaka Hospital Ethics Committee (approval ID: 2016-2), Kobe Ekisaikai Hospital Ethics Committee (approval ID: 2016-3), Sakurabashi Watanabe Hospital Ethics Committee (approval ID: 16-15), Sumitomo Hospital Research Ethics Committee (approval ID: 28-01), Suita Municipal Hospital Institutional Review Board (approval ID: 2017-8), Kinki Central Hospital Ethics Committee (approval ID: 288), Osaka Police Hospital Institutional Review Board (approval ID: 593), Japan Community Health Care Organization Hoshigaoka Medical Center Institutional Review Board (approval ID: 1618), National Hospital Organization Osaka Minami Medical Center Institutional Review Board (approval ID: 28-3), Japan Community Health Care Organization Osaka Minato Central Hospital Ethics Committee (approval ID unvailable, but approved on 10 June 2016), Amagasaki Chuo Hospital Ethics Committee (approval ID unavailable, but approved on 1 Aug 2017), Otemae Hospital Institutional Review Board (approval ID: 2017-020), Osaka University Hospital Clinical Research Review Committee (approval ID: 15471), Osaka International Cancer Institute Institutional Review Board (No.20097).
Figures






References
-
- Chinnaiyan KM, Alexander D, Maddens M, McCullough PA (2007) Curriculum in cardiology: integrated diagnosis and management of diastolic heart failure. Am Heart J 153(2):189–200 - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM (2006) Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 355(3):251–259 - PubMed
-
- Anker SD, Butler J, Filippatos G, Ferreira JP, Bocchi E, Böhm M, Brunner-La Rocca HP, Choi DJ, Chopra V, Chuquiure-Valenzuela E, Giannetti N, Gomez-Mesa JE, Janssens S, Januzzi JL, Gonzalez-Juanatey JR, Merkely B, Nicholls SJ, Perrone SV, Piña IL, Ponikowski P, Senni M, Sim D, Spinar J, Squire I, Taddei S, Tsutsui H, Verma S, Vinereanu D, Zhang J, Carson P, Lam CSP, Marx N, Zeller C, Sattar N, Jamal W, Schnaidt S, Schnee JM, Brueckmann M, Pocock SJ, Zannad F, Packer M (2021) Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med 385(16):1451–1461 - PubMed
-
- Senni M, Paulus WJ, Gavazzi A, Fraser AG, Díez J, Solomon SD, Smiseth OA, Guazzi M, Lam CS, Maggioni AP, Tschöpe C, Metra M, Hummel SL, Edelmann F, Ambrosio G, Stewart Coats AJ, Filippatos GS, Gheorghiade M, Anker SD, Levy D, Pfeffer MA, Stough WG, Pieske BM (2014) New strategies for heart failure with preserved ejection fraction: the importance of targeted therapies for heart failure phenotypes. Eur Heart J 35(40):2797–2815 - PMC - PubMed
-
- Kinugasa Y, Kato M, Sugihara S, Hirai M, Yamada K, Yanagihara K, Yamamoto K (2013) Geriatric nutritional risk index predicts functional dependency and mortality in patients with heart failure with preserved ejection fraction. Circ J 77(3):705–711 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
