

A multidisciplinary comprehensive nursing Management Approach for Catheter-related bloodstream infections
- PMID: 39656345
- PMCID: PMC11754313
- DOI: 10.1007/s10096-024-05002-7
A multidisciplinary comprehensive nursing Management Approach for Catheter-related bloodstream infections
Abstract
Background: Catheter-related bloodstream infection (CR-BSI) stands as one of the leading causes of hospital-acquired infections, often resulting in high healthcare expenditure and mortality rates. Despite efforts, reducing the incidence of CR-BSI remains a significant challenge.
Objective: This study aimed to assess the impact of a multidisciplinary organizational intervention on reducing intravenous CR-BSI.
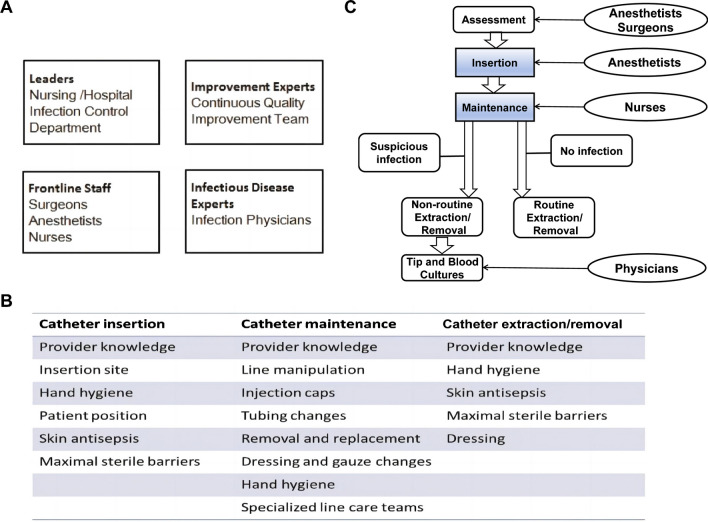
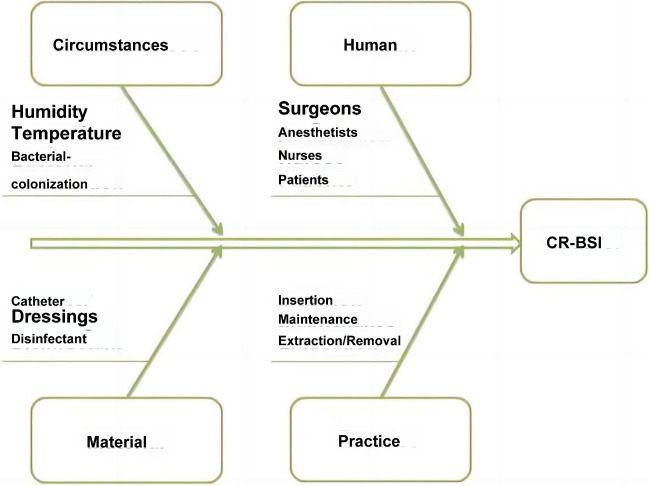
Methods: A quality improvement team was established to implement various interventions, utilizing the FOCUS-PDCA continuous quality improvement model and fishbone diagram for analysis and improvement.
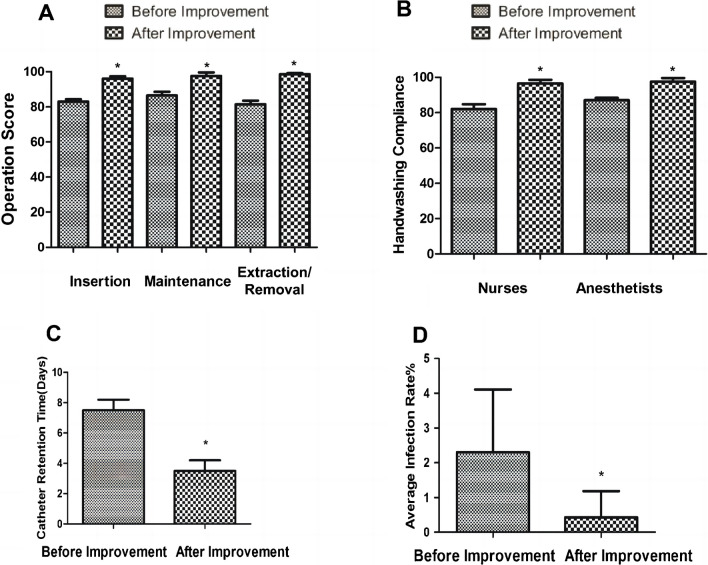
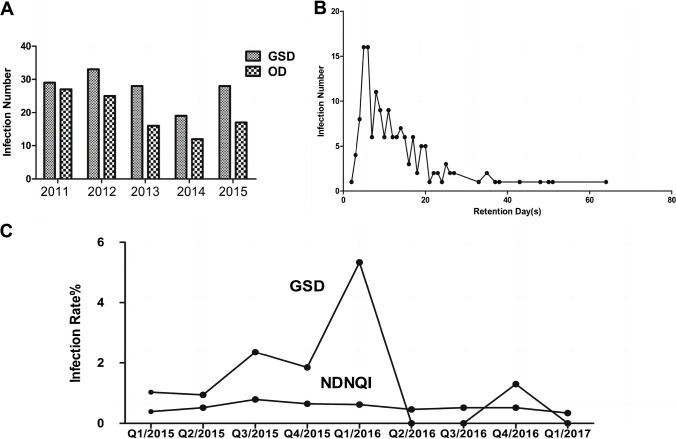
Results: After the interventions, operational indicators for catheter insertion, maintenance, and removal improved from 82.50% ± 1.15%, 83.60% ± 1.60%, and 81.60% ± 1.80-95.30% ± 1.00%, 96.20% ± 1.62%, and 97.25% ± 0.50%, respectively. Additionally, catheter dwell time decreased from 7.50 ± 0.85 days to 3.50 ± 0.75 days, and the quarterly infection rate was reduced from 2.328% ± 1.85-0.305% ± 0.95% following the implementation of the intervention.
Discussion: Despite the available evidence, there remains a noticeable gap between the ideal evidence-based practices and their practical implementation. We aim to eradicate CR-BSIs within the surgical intensive care units (ICUs) of hospitals. To achieve this goal, we have introduced a comprehensive quality improvement framework designed not only to benefit our own ICU but also to serve as a model for implementation in other similar healthcare settings.
Keywords: Central venous line; Continuous quality improvement; General surgical nursing departments; Nosocomial infection; Organizational creativity.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interests The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article. Ethical approval: Not applicable.
Figures
References
-
- Lutwick L et al (2019) Managing and preventing vascular catheter infections: a position paper of the international society for infectious diseases. Int J Infect Dis 84:22–29 - PubMed
-
- Pronovost PJ, Marsteller JA, Goeschel CA (2011) Preventing bloodstream infections: a measurable national success story in quality improvement. Health Aff 30:628–634 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
