

Renal venous flow in different regions of the kidney are different and reflecting different etiologies of venous reflux disorders in septic acute kidney injury: a prospective cohort study
- PMID: 39656352
- PMCID: PMC11631833
- DOI: 10.1186/s40635-024-00700-0
Renal venous flow in different regions of the kidney are different and reflecting different etiologies of venous reflux disorders in septic acute kidney injury: a prospective cohort study
Abstract
Background: Acute kidney injury (AKI) is a frequent complication of sepsis. While impaired renal venous reflux indicates renal congestion, the relationship between AKI outcomes and hemodynamic parameters remains debated. This study aimed to investigate the utility of renal venous flow patterns in various regions of septic patients and to explore the association between hemodynamic parameters and renal function prognosis.
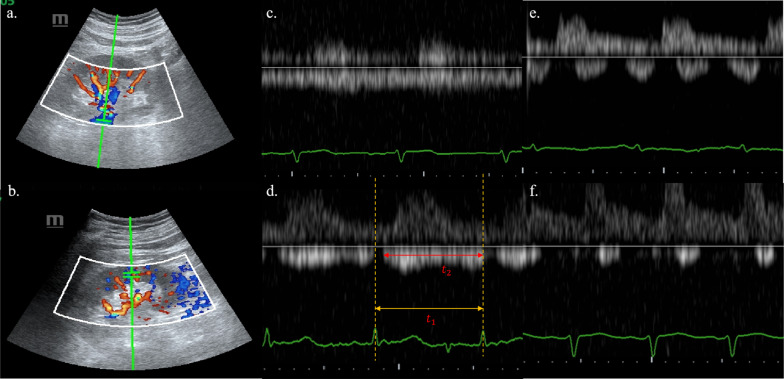
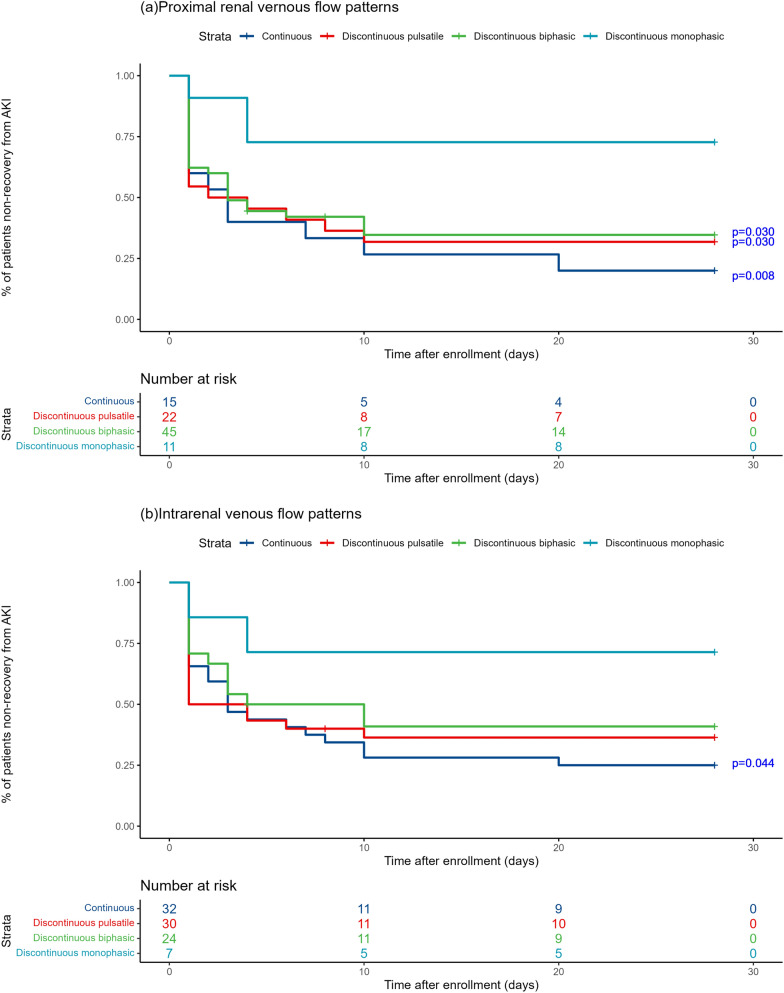
Methods: In this single-center, prospective longitudinal study, adult sepsis patients diagnosed with AKI were enrolled. Renal ultrasonography was performed within 24 h of ICU admission (D1), then repeated at D3 and D5. Patterns of proximal renal venous flow (PRVF) and intrarenal venous flow (IRVF) patterns were confirmed by two blinded sonographers. Kaplan-Meier survival analysis was used to evaluate renal prognosis, and cumulative incidence curves were generated for renal function recovery time.
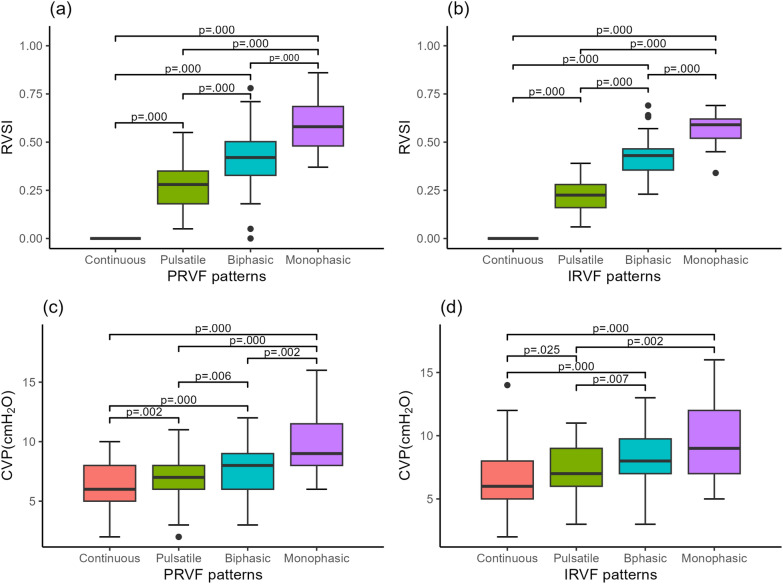
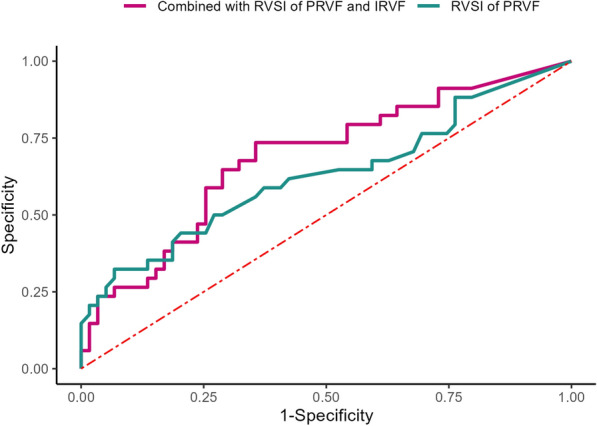
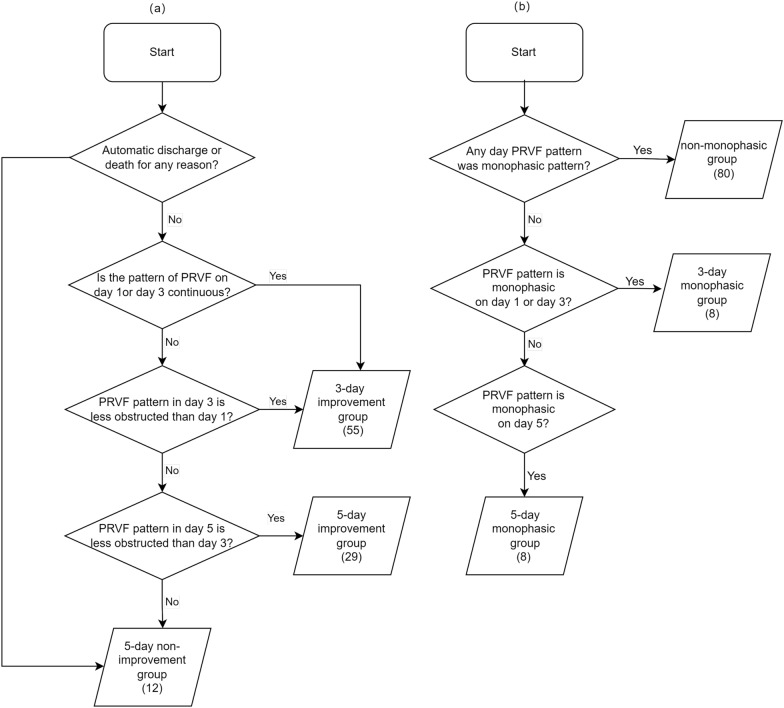
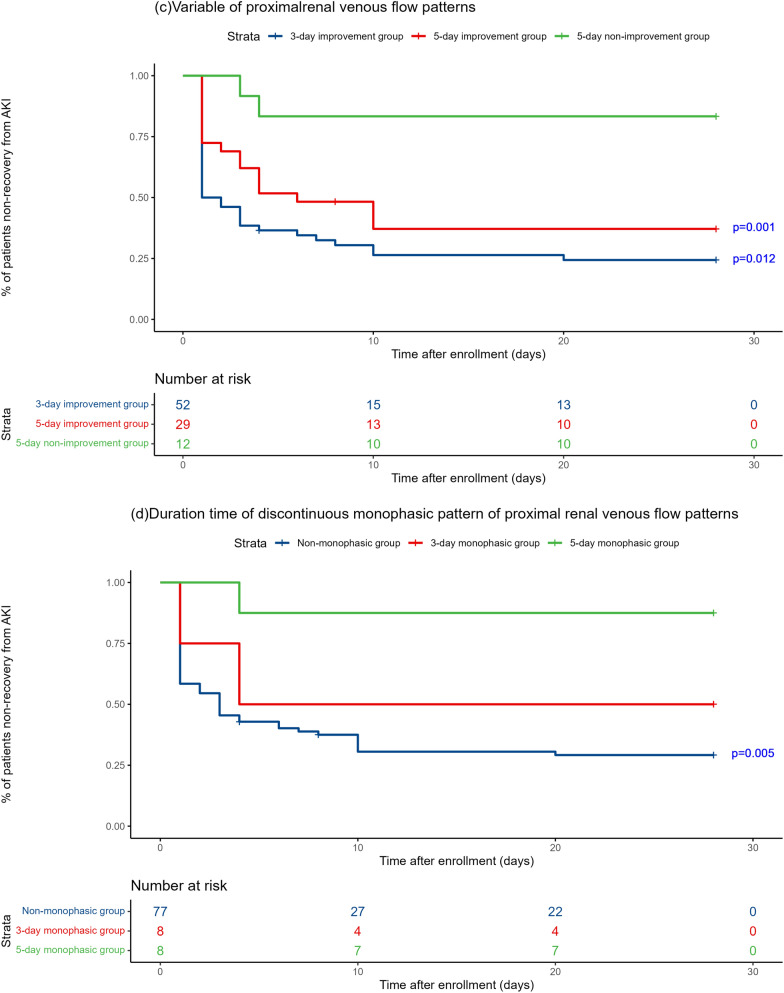
Results: The study included 96 septic patients. Inconsistencies between PRVF and IRVF patterns occurred in 31.9%, with PRVF patterns being more severe in 88% of these. A relatively strong correlation was observed between PRVF and CVP, but this trend was less evident in IRVF. For RVSI of PRVF at ICU admission, the AUC to predict 28-day renal function prognosis was 0.626 (95% CI 0.502-0.750, P = 0.044), while combined PRVF and IRVF had a higher predictive ability (AUC 0.687, 95% CI 0.574-0.801, P = 0.003). The 28-day renal prognosis was poorer in the PRVF 5-day non-improvement group compared to the 3-day improvement group (P = 0.001) and 5-day improvement group (P = 0.012). Patients with a persistent monophasic PRVF pattern within 5 days had a worse prognosis than the non-monophasic group (P = 0.005).
Conclusions: Our study reveals that patterns of PRVF and IRVF are not entirely congruent, stepwise evaluation is useful in determining the intervention site for renal vein reflux disorders. Combined PRVF and IRVF had a higher predictive ability for 28-day renal function prognosis. Early improvement in renal venous congestion is crucial for better renal function prognosis. This study is registered with ClinicalTrials.gov, number NTC06159010. Retrospectively registered 28 November 2023.
Keywords: Acute kidney injury; Intrarenal venous flow; Proximal renal venous flow; Renal congestion; Sepsis.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was designed as a single-center prospective study conducted at Peking Union Medical College Hospital. The protocol was approved by the Ethics Committee of Peking Union Medical College Hospital (approval number I-23PJ176). Written informed consents were obtained from all participants. Consent for publication: Not applicable. Competing interests: On behalf of all authors, the corresponding author declares that there are no conflicts of interest.
Figures


References
-
- Bhardwaj V, Vikneswaran G, Rola P, Raju S, Bhat RS, Jayakumar A, Alva A (2020) Combination of inferior vena cava diameter, hepatic venous flow, and portal vein pulsatility index: venous excess ultrasound score (VEXUS Score) in predicting acute kidney injury in patients with cardiorenal syndrome: a prospective cohort study. Indian J Crit Care Med 24(9):783–789 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
