

Audit and Feedback Interventions for Antibiotic Prescribing in Primary Care: A Systematic Review and Meta-analysis
- PMID: 39657007
- PMCID: PMC11848270
- DOI: 10.1093/cid/ciae604
Audit and Feedback Interventions for Antibiotic Prescribing in Primary Care: A Systematic Review and Meta-analysis
Abstract
Background: This systematic review evaluates the effect of audit and feedback (A&F) interventions targeting antibiotic prescribing in primary care and examines factors that may explain the variation in effectiveness.
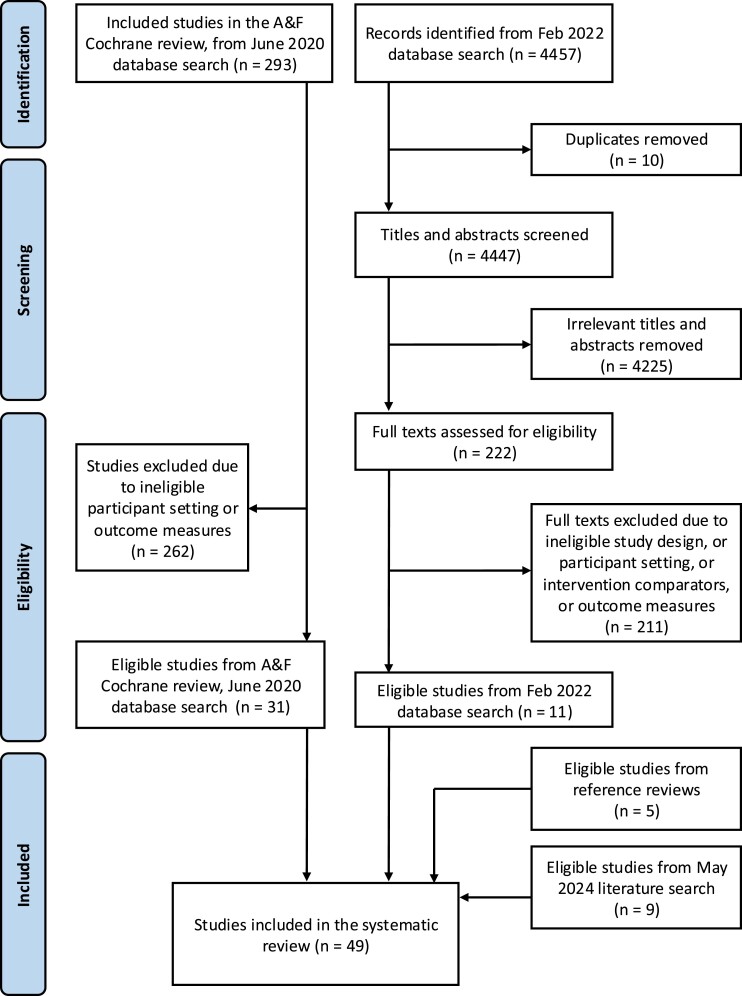
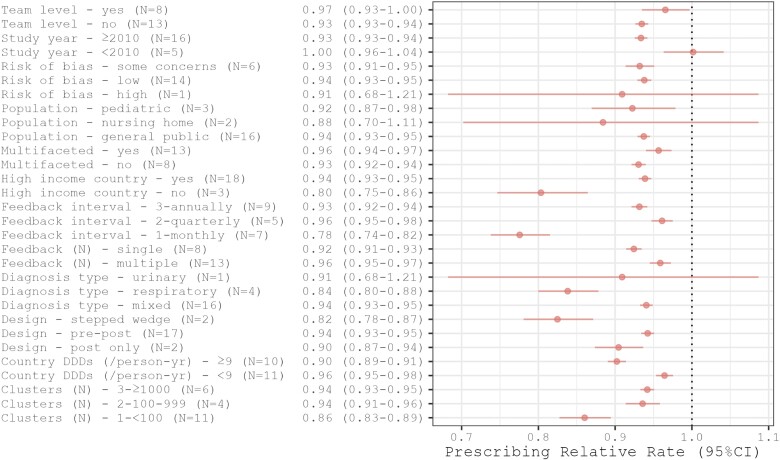
Methods: Randomized controlled trials (RCTs) involving A&F interventions targeting antibiotic prescribing in primary care were included in the systematic review. Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, CINAHL, and ClinicalTrials.gov were searched up to May 2024. Trial, participant, and intervention characteristics were extracted independently by 2 researchers. Random effects meta-analyses of trials that compared interventions with and without A&F were conducted for 4 outcomes: (1) total antibiotic prescribing volume; (2) unnecessary antibiotic initiation; (3) excessive prescription duration, and (4) broad-spectrum antibiotic selection. A stratified analysis was also performed based on study characteristics and A&F intervention design features for total antibiotic volume.
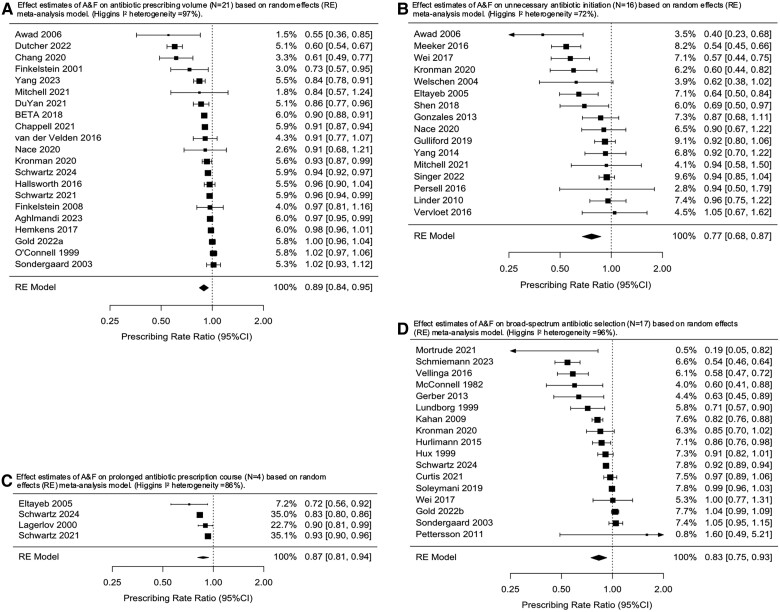
Results: A total of 56 RCTs fit the eligibility criteria and were included in the meta-analysis. A&F was associated with an 11% relative reduction in antibiotic prescribing volume (N = 21 studies, rate ratio [RR] = 0.89; 95% confidence interval [CI]: .84, .95; I2 = 97); 23% relative reduction in unnecessary antibiotic initiation (N = 16 studies, RR = 0.77; 95% CI: .68, .87; I2 = 72); 13% relative reduction in prolonged duration of antibiotic course (N = 4 studies, RR = 0.87 95% CI: .81, .94; I2 = 86); and 17% relative reduction in broad-spectrum antibiotic selection (N = 17 studies, RR = 0.83 95% CI: .75, .93; I2 = 96).
Conclusions: A&F interventions reduce antibiotic prescribing in primary care. However, heterogeneity was substantial, outcome definitions were not standardized across the trials, and intervention fidelity was not consistently assessed. Clinical Trials Registration. Prospero (CRD42022298297).
Keywords: antibiotics; audit and feedback; primary care; systematic review.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. The authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Society for Healthcare Epidemiology of America, Infectious Diseases Society of America, Pediatric Infectious Diseases Society . Policy statement on antimicrobial stewardship by the Society for Healthcare Epidemiology of America (SHEA), the Infectious Diseases Society of America (IDSA), and the Pediatric Infectious Diseases Society (PIDS). Infect Control Hosp Epidemiol 2012; 33:322–7. - PubMed
-
- Duffy E, Ritchie S, Metcalfe S, Van Bakel B, Thomas MG. Antibacterials dispensed in the community comprise 85%–95% of total human antibacterial consumption. J Clin Pharm Ther 2018; 43:59–64. - PubMed
-
- Hawker JI, Smith S, Smith GE, et al. Trends in antibiotic prescribing in primary care for clinical syndromes subject to national recommendations to reduce antibiotic resistance, UK 1995–2011: analysis of a large database of primary care consultations. J Antimicrob Chemother 2014; 69:3423–30. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL167023/HL/NHLBI NIH HHS/United States
- R01 AG069762/AG/NIA NIH HHS/United States
- U01 NS105562/NS/NINDS NIH HHS/United States
- R01 HS024930/HS/AHRQ HHS/United States
- R01 HS029328/HS/AHRQ HHS/United States
- R01 AG070054/AG/NIA NIH HHS/United States
- U19 AG065188/AG/NIA NIH HHS/United States
- R24 AG064025/AG/NIA NIH HHS/United States
- R21 AG081895/AG/NIA NIH HHS/United States
- FRN 173704/CIHR/Canada
- R01 AG074245/AG/NIA NIH HHS/United States
- P30 AG059988/AG/NIA NIH HHS/United States
- P30 AG024968/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
