

Higher risk profile among patients with TET2-mutated giant cell arteritis: a cluster analysis
- PMID: 39658053
- PMCID: PMC11647381
- DOI: 10.1136/rmdopen-2024-004694
Higher risk profile among patients with TET2-mutated giant cell arteritis: a cluster analysis
Abstract
Objective: We aimed to assess the prevalence of clonal haematopoiesis (CH) in patients with giant cell arteritis (GCA) compared with controls and individuals with other autoimmune diseases (AIDs) and to identify high-risk clinical/genetic profiles that could influence disease outcomes.
Methods: In a prospective observational study at three hospitals, we included 49 patients diagnosed with GCA, 48 patients with other AIDs and 27 control participants. We used next-generation sequencing to detect clonal haematopoiesis (CH) among them.
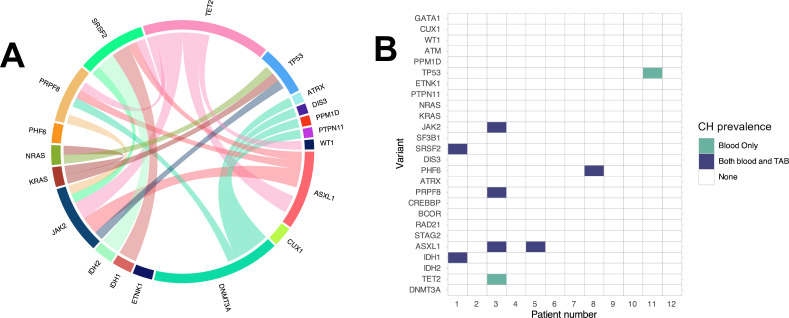
Results: CH was detected in 55.1% of patients with GCA, 59.3% of controls and 18.8% of patients with other AIDs. The most commonly mutated genes in GCA and control groups were DNMT3A and TET2. No significant differences in CH prevalence were found between patients with GCA and controls or other AID when adjusted for age and sex. Cluster analysis revealed two distinct groups within the patients with GCA, one of which displayed a higher prevalence of TET2 and JAK2 variants, and was associated with worse prognosis.
Conclusions: CH is prevalent among patients with GCA but does not differ significantly from controls or other autoimmune conditions. However, specific genetic profiles, particularly mutations in TET2 and JAK2, are associated with a higher risk cluster within the GCA cohort. This observation highlights the interest of detecting CH in patients with GCA in both routine practice and clinical trials for better risk stratification. Further prospective studies are needed to determine if management tailored to the genetic profile would improve outcomes.
Keywords: epidemiology; giant cell arteritis; vasculitis.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous