

Human papillomavirus genotype-specific prevalence and infection risks: a 10-year population-based study from the United States
- PMID: 39658224
- PMCID: PMC12058271
- DOI: 10.1093/jnci/djae327
Human papillomavirus genotype-specific prevalence and infection risks: a 10-year population-based study from the United States
Abstract
Background: Various studies have reported on the impact of human papillomavirus (HPV) vaccines. Here we present the largest population-based investigation of genotype-specific distributions over the decade following implementation of the quadrivalent HPV vaccine (HPV-6/11/16/18) in the United States.
Methods: Liquid-based cervical cytology samples from individuals aged 15-30 years undergoing cervical screening throughout New Mexico were tested by broad-spectrum HPV genotyping. Weighted relative differences in HPV type-specific prevalence and 95% confidence intervals (CIs) were calculated by comparing individuals screened between 2007 and 2009 (n = 95 915) with individuals screened between 2013 and 2016 (n = 103 371). Weighted logistic regression was used to estimate relative risk of type-specific HPV infections. Tests of significance were 2-sided.
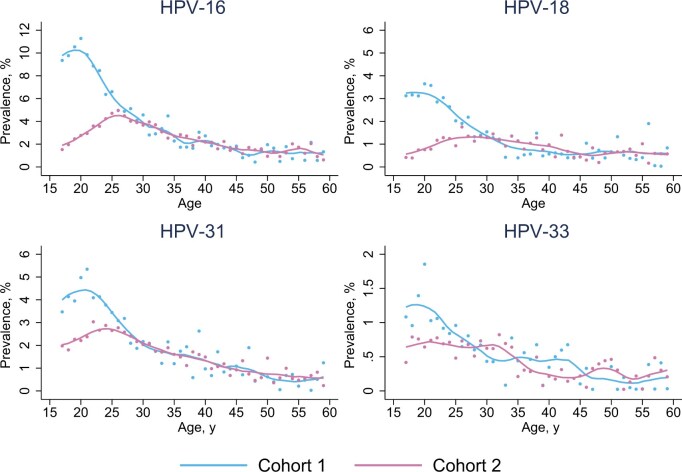
Results: Genotype-specific prevalence fell with statistical signficance for HPV-16 (relative difference = ‒52.6%, 95% CI = ‒56.9 to ‒48.3), HPV-18 (relative difference = ‒62.1%, 95% CI = ‒68.5 to ‒55.8), HPV-31 (relative difference = ‒34.2%, 95% CI = ‒42.1 to ‒26.3), and HPV-33 (relative difference = ‒31.8%, 95% CI = ‒48.4 to ‒15.1). The relative difference increased for other carcinogenic HPV types by 19.5% (95% CI = 14.3 to 24.6) when excluding HPV-16/18. Large reductions in HPV-6/11 relative differences were observed, but overall, noncarcinogenic, nonvaccine types increased. Comparing female individuals born in 1996 with female individuals born in 1989, risk of infection with HPV-6, 11, 16, and 18 decreased by 80.0% among individuals aged 21-25 years. High-grade squamous intraepithelial lesions or worse decreased by 49.4% when extending the evaluation from 2007 to 2018.
Conclusion: The incidence of high-grade squamous intraepithelial lesions or worse is decreasing, with large reductions in the prevalence of quadrivalent HPV vaccine types and nonvaccine types HPV-31 and HPV-33, reflecting vaccine cross-protection. Increases in nonvaccine HPV genotypes may attenuate anticipated reductions in HPV-related abnormalities, including cancers, but the benefits of HPV vaccination remain substantial.
© The Author(s) 2024. Published by Oxford University Press.
Conflict of interest statement
C.M.W. and J.C. have received funds from grants, cooperative agreements, or subcontracts related to cervical screening and triage through their respective institutions, the University of New Mexico Health Sciences Center and Queen Mary University London. C.M.W. reports receiving reagents and equipment from Roche Molecular Systems, Roche/Ventana Medical Systems, and Hologic through her institution and outside the submitted work as well as research support from Hologic and Becton Dickinson, also outside this work. J.C. reports being on the speaker’s bureau for Hologic and Becton Dickinson and the data monitoring committee for a Roche liver cancer trial. Dr Stoler is a consultant in clinical trial development and performance and an expert pathologist in clinical trials for Merck, Roche/Ventana Medical Systems, Becton Dickinson Life Sciences, Abbott Molecular, Inovio Pharmaceuticals, and Frantz Viral Therapeutics. P.E.C., who is a
Figures



References
-
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209-249. - PubMed
-
- World Health Organisation. Cervical cancer. Accessed January 26, 2025. https://www.who.int/health-topics/cervical-cancer
-
- Smith JS, Lindsay L, Hoots B, et al. Human papillomavirus type distribution in invasive cervical cancer and high-grade cervical lesions: a meta-analysis update. Int J Cancer. 2007;121:621-632. - PubMed
-
- Saslow D, Andrews KS, Manassaram-Baptiste D, et al. ; American Cancer Society Guideline Development Group. Human papillomavirus vaccination 2020 guideline update: American Cancer Society guideline adaptation. CA Cancer J Clin. 2020;70:274-280. - PubMed
