

Investigation of left ventricular ejection fraction in a Swiss heart failure population: Insights into mortality and sex differences
- PMID: 39658884
- PMCID: PMC12055381
- DOI: 10.1002/ehf2.15174
Investigation of left ventricular ejection fraction in a Swiss heart failure population: Insights into mortality and sex differences
Abstract
Aims: Understanding heart failure (HF) characteristics is essential to improve patient outcomes. Categorizing HF beyond left ventricular ejection fraction (LVEF) is challenging due to heterogeneous clinical presentation and aetiologies. Despite global studies on HF, the role of LVEF on mortality remains controversial. We explored the association of LVEF with mortality, considering sex differences and comorbidities in a cohort from the largest tertiary cardiovascular centre in Switzerland.
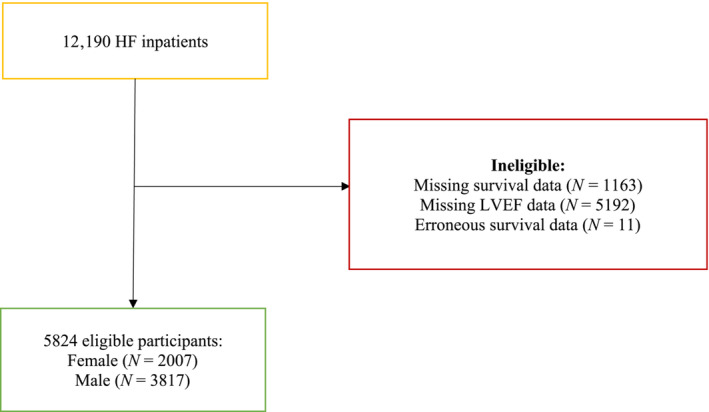
Methods: HF patients admitted to the University Hospital of Bern from January 2015 to December 2019 were evaluated. LVEF was used to classify patients into HF with preserved ejection fraction (HFpEF), HF with mid-range ejection fraction (HFmrEF) and HF with reduced preserved ejection fraction (HFrEF) categories. Cox proportional hazard models and time-stratified analyses adjusted for potential confounders were employed.
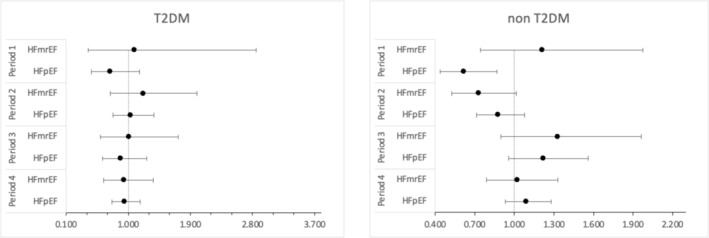
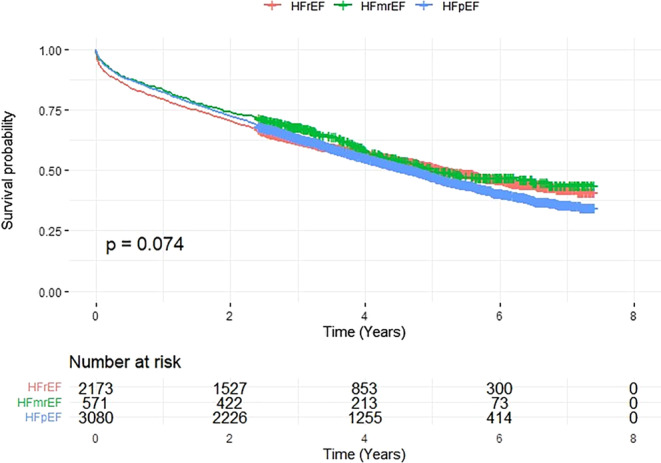
Results: A total of 5824 HF patients were included, and 2912 died over a median follow-up time of 3.39 years. Mortality rates across LVEF categories showed no significant differences, while overall, women showed significantly higher mortality; 30 day mortality was lower in the HFpEF category [hazard ratio (HR) 0.67, 95% confidence interval (CI): 0.52-0.88, P = 0.003], with persistent effects upon stratification in males (HR 0.59, 95% CI: 0.42-0.81, P < 0.001) and non-diabetics (HR 0.62, 95% CI: 0.44-0.87, P = 0.005). An isolated reduction in HFpEF mortality was observed in females after 1 year (HR 0.72, 95% CI: 0.53-0.98, P = 0.035).
Conclusions: The prognostic role of LVEF on all-cause mortality remains unclear, while differences in mortality rate distribution between women and men mirror established HF pathophysiological sex differences. Future HF studies should focus on HF aetiology and include measures beyond LVEF for comprehensive characterization.
Keywords: heart failure; sex differences.
© 2024 The Author(s). ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
Taulant Muka works at Epistudia GmbH and acts as an unpaid advisor for the Academic Parity Movement, a non‐profit organization uprooting academic bullying and discrimination. The other authors declare that they have no conflicts of interest.
Figures


References
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators . Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018;392:1789‐1858. doi:10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
