

Association of systemic immune-inflammation index with all-cause and cardio-cerebrovascular mortality in individuals with diabetic kidney disease: evidence from NHANES 1999-2018
- PMID: 39659615
- PMCID: PMC11628304
- DOI: 10.3389/fendo.2024.1399832
Association of systemic immune-inflammation index with all-cause and cardio-cerebrovascular mortality in individuals with diabetic kidney disease: evidence from NHANES 1999-2018
Abstract
Background: Emerging evidence suggests a potential role of immune response and inflammation in the pathogenesis of diabetic kidney disease (DKD). The systemic immune-inflammation index (SII) offers a comprehensive measure of inflammation; however, its relationship with the prognosis of DKD patients remains unclear.
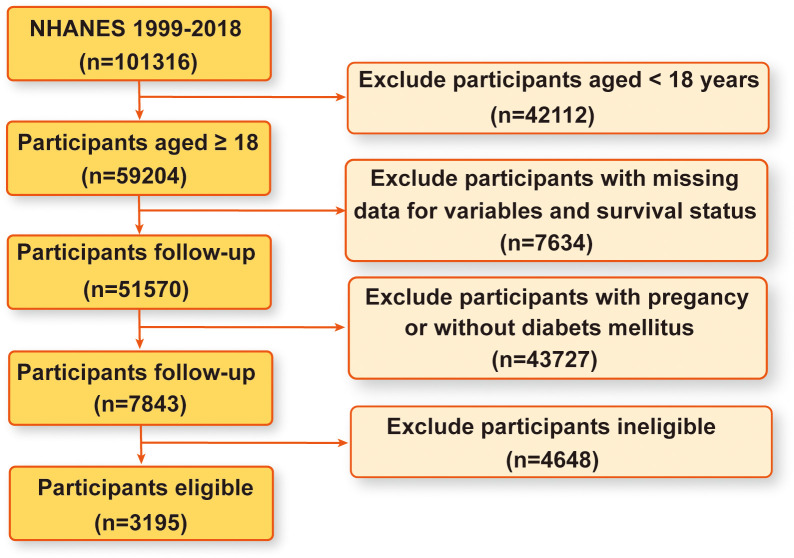
Methods: Using data from the National Health and Nutrition Examination Survey (NHANES) spanning 1999 to 2018, this cross-sectional study involved adults diagnosed with DKD. Cox proportional hazards models were utilized to assess the associations between SII and all-cause or cardio-cerebrovascular disease mortality. Additionally, restricted cubic spline, piecewise linear regression, and subgroup analyses were performed.
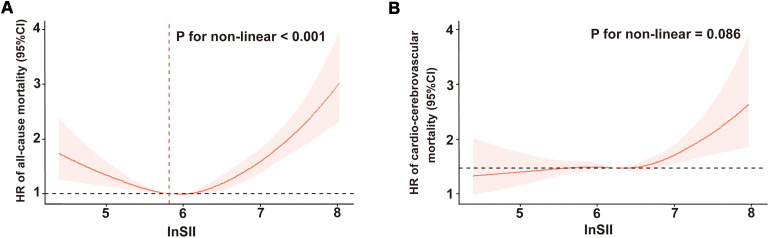
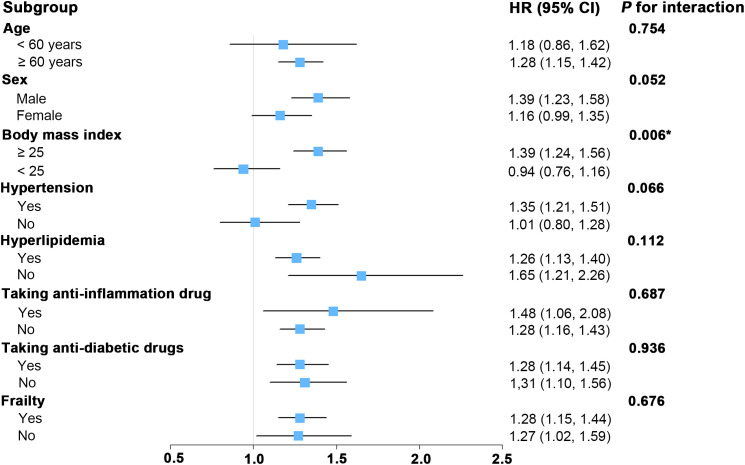
Results: Over a median follow-up duration of 6.16 years, 1338 all-cause deaths were recorded. After adjusting for covariates, elevated SII levels were significantly associated with increased risks of all-cause and cardio-cerebrovascular disease mortality. Specifically, per one-unit increment in natural log-transformed SII (lnSII), there was a 29% increased risk of all-cause mortality (P < 0.001) and a 23% increased risk of cardio-cerebrovascular disease mortality (P = 0.01) in the fully adjusted model. Similar results were observed when SII was analyzed as a categorical variable (quartiles). Moreover, nonlinear association was identified between SII and all-cause mortality (P < 0.001) through restricted cubic spline analysis, with threshold value of 5.82 for lnSII. The robustness of these findings was confirmed in subgroup analyses. Likewise, the statistically significant correlation between SII levels and cardio-cerebrovascular disease mortality persisted in individuals with DKD.
Conclusion: Increased SII levels, whether examined as continuous variables or categorized, demonstrate a significant association with elevated risks of all-cause and cardio-cerebrovascular disease mortality among DKD patients. These findings imply that maintaining SII within an optimal range could be crucial in reducing mortality risk.
Keywords: NHANES; all-cause mortality; cardio-cerebrovascular disease mortality; diabetes mellitus; diabetic kidney disease; population-based study; systemic immune-inflammation index.
Copyright © 2024 Zhang, Ye, Li, Zhang, Tan, Wang, Xie, Peng, Li, Chen, Wen, Chan, Tang, Li and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Association of systemic immune inflammatory index with all-cause and cause-specific mortality in hypertensive individuals: Results from NHANES.Front Immunol. 2023 Feb 2;14:1087345. doi: 10.3389/fimmu.2023.1087345. eCollection 2023. Front Immunol. 2023. PMID: 36817427 Free PMC article.
-
Systemic immune-inflammation index (SII) and the risk of all-cause, cardiovascular, and cardio-cerebrovascular mortality in the general population.Eur J Med Res. 2023 Dec 9;28(1):575. doi: 10.1186/s40001-023-01529-1. Eur J Med Res. 2023. PMID: 38066657 Free PMC article.
-
The aggregate index of systemic inflammation (AISI) and the risk of all-cause, cardiovascular, and cardio-cerebrovascular mortality in congestive heart failure patients: results from NHANES 1999-2018.Sci Rep. 2025 May 26;15(1):18282. doi: 10.1038/s41598-025-01196-8. Sci Rep. 2025. PMID: 40414913 Free PMC article.
-
Relationship between systemic immune inflammation index and mortality among US adults with different diabetic status: Evidence from NHANES 1999-2018.Exp Gerontol. 2024 Jan;185:112350. doi: 10.1016/j.exger.2023.112350. Epub 2023 Dec 22. Exp Gerontol. 2024. PMID: 38128848
-
Association Between Systemic Immune-Inflammation Index and Psoriasis, Psoriasis Comorbidities, and All-Cause Mortality: A Study Based on NHANES.Immun Inflamm Dis. 2024 Oct;12(10):e70050. doi: 10.1002/iid3.70050. Immun Inflamm Dis. 2024. PMID: 39467182 Free PMC article. Review.
Cited by
-
Associations of serum Klotho with diabetic kidney disease prevalence and mortality: insights from a nationally representative U.S. cohort.Diabetol Metab Syndr. 2025 Jun 7;17(1):198. doi: 10.1186/s13098-025-01729-1. Diabetol Metab Syndr. 2025. PMID: 40481564 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical