

Terbinafine in acrylic polymer for the treatment of onychomycosis in hemodialysis patients: a phase II clinical trial
- PMID: 39659625
- PMCID: PMC11628268
- DOI: 10.3389/fmed.2024.1417985
Terbinafine in acrylic polymer for the treatment of onychomycosis in hemodialysis patients: a phase II clinical trial
Abstract
Introduction: Onychomycosis is a nail infection caused by dermatophyte fungi, non-dermatophyte fungi, and yeast. Patients with chronic kidney disease on dialysis are part of the population that presents higher rates of this disease, mainly due to immunosuppression. Among patients with chronic kidney disease on dialysis, the treatment of onychomycosis is complex, mainly due to the limitations imposed by comorbidities. In this context, the study evaluated the safety and potential efficacy of a treatment that combines nail debridement with the use of acrylic gel nails carrying terbinafine at a concentration of 2%.
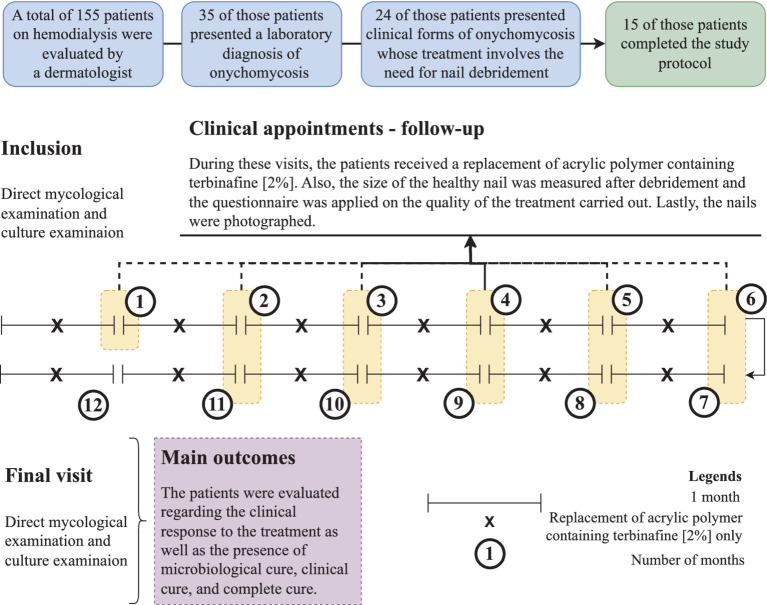
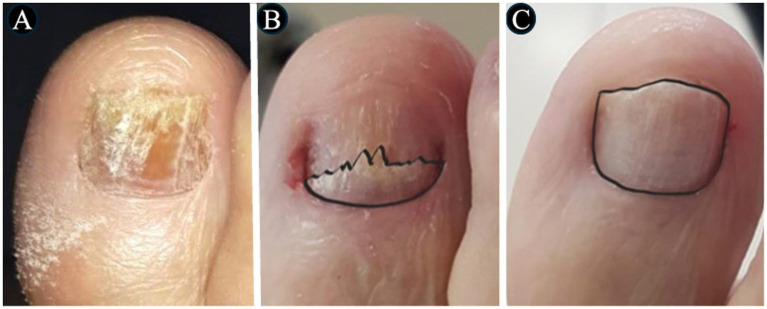
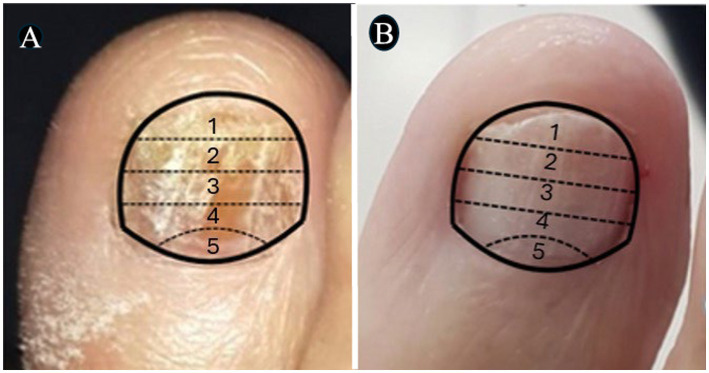
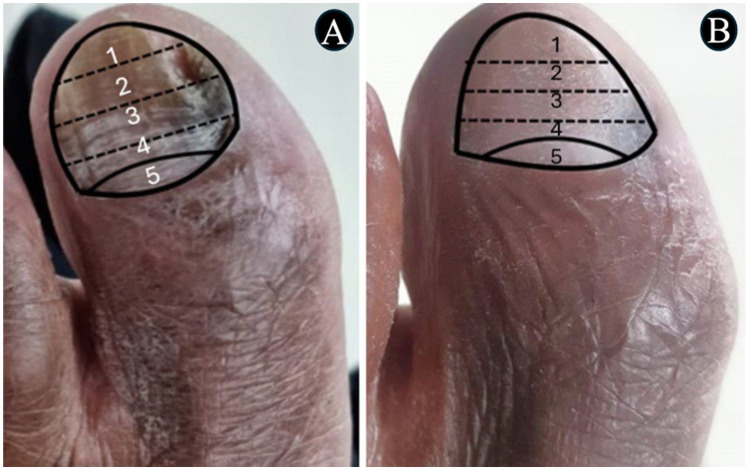
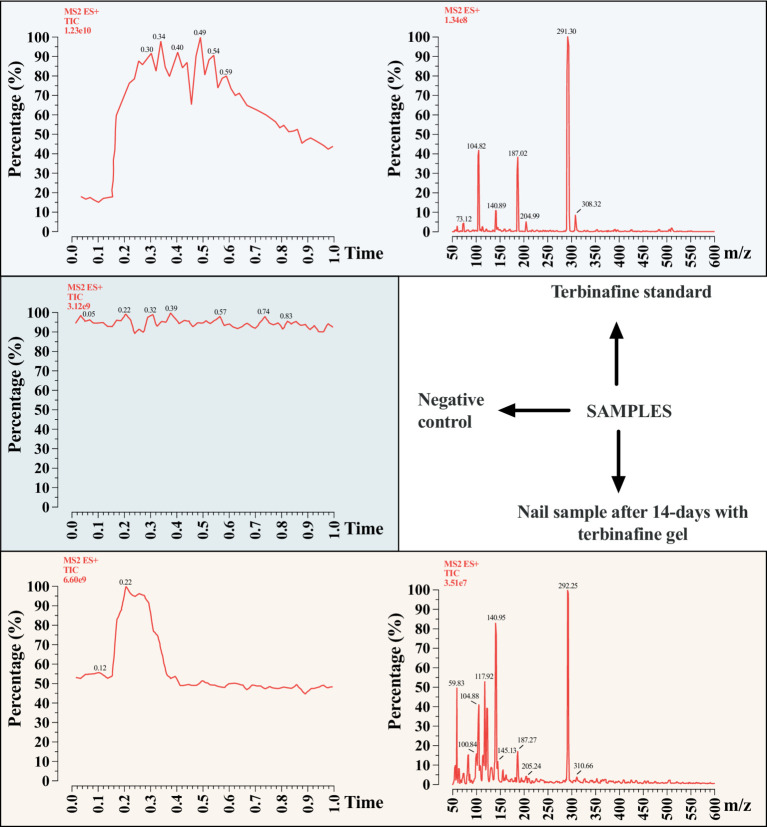
Methods: Patients from the Hemodialysis Center of the São Francisco de Assis University Hospital in Bragança Paulista, São Paulo, Brazil were included. Those had hallux onychomycosis with clinical forms whose treatment involved the need for nail debridement. After the debridement procedure, a nail prosthesis made with acrylic reconstruction gel and 2% terbinafine was applied. The procedure was renewed every 2 weeks (~14 days) for 11 months. The evolution was monitored with measurements of the normal-appearing nail plate and photographs. Direct mycological examination and fungal culture were performed at the beginning of the study and 30 days after applications were interrupted. Assessment of clinical response, clinical cure, mycological cure, and complete cure was performed at the end of the study. All participants answered a questionnaire about their perception of the treatment.
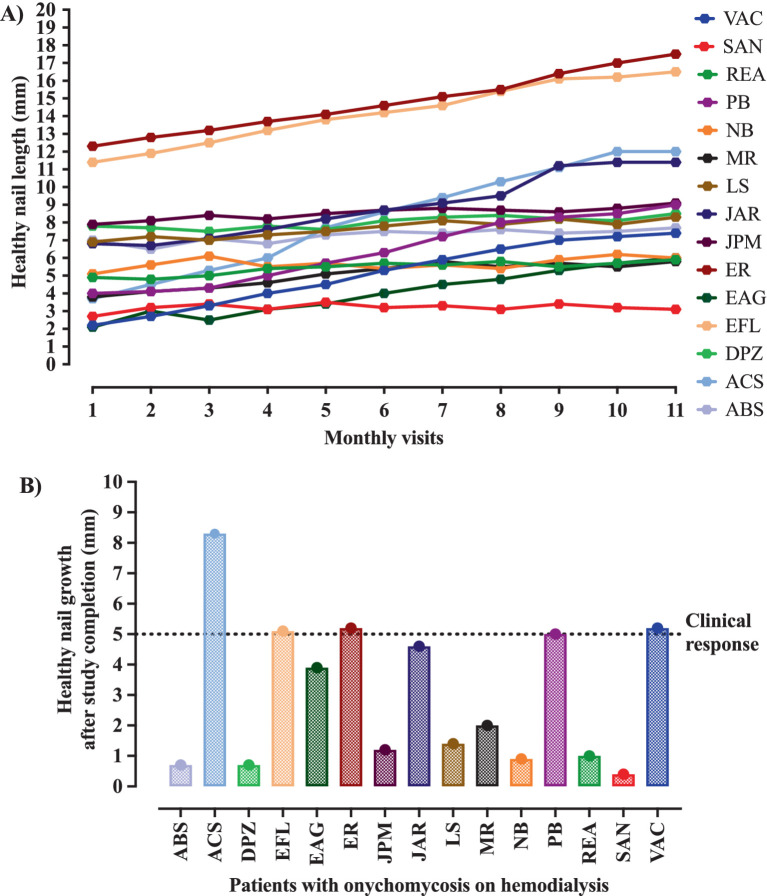
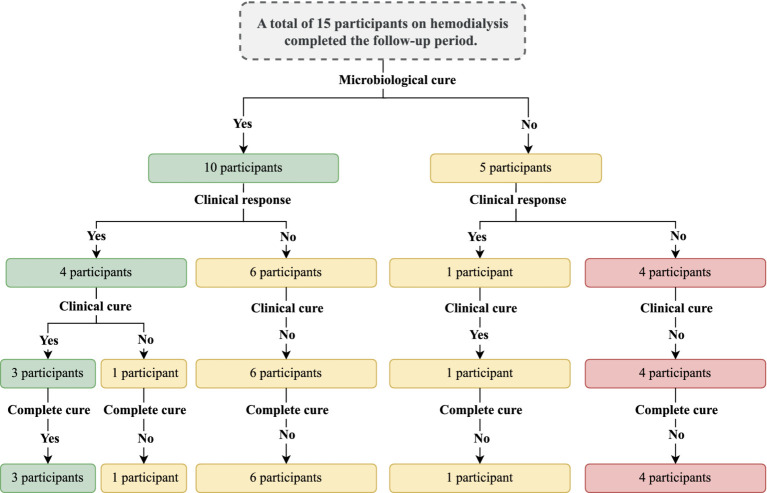
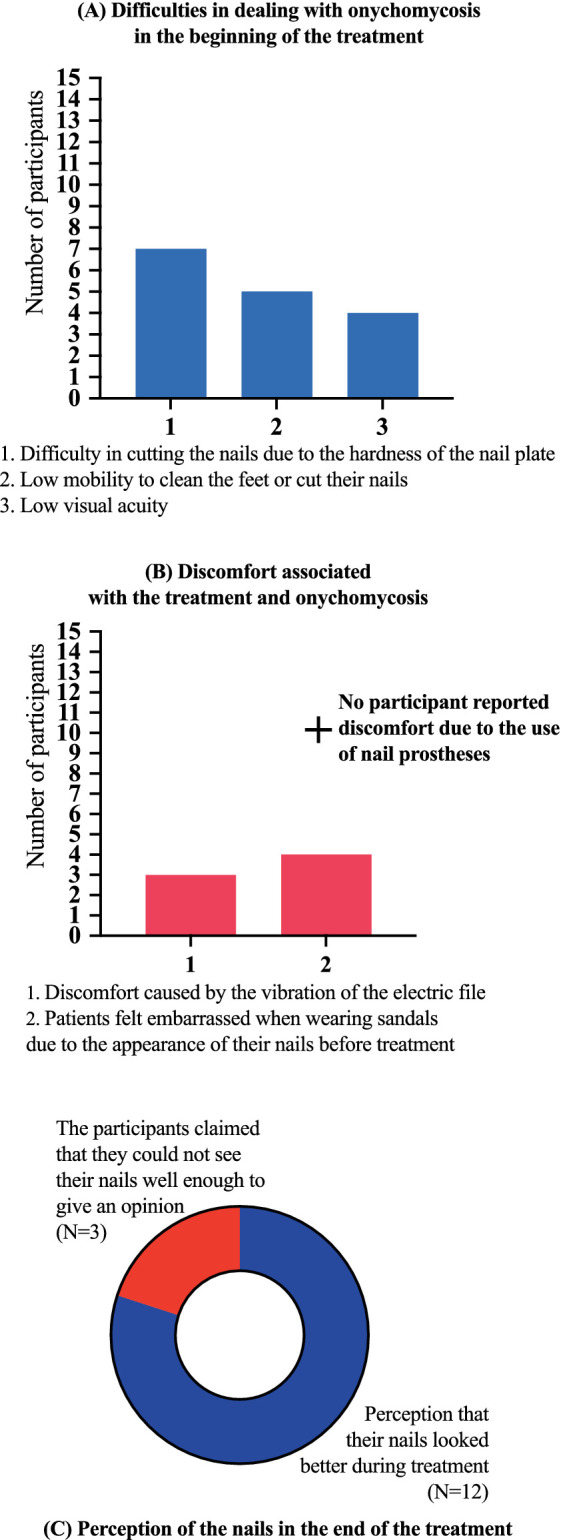
Results: Out of the 155 patients on hemodialysis, 64/155 (41.3%) individuals were identified with symptoms suggestive of onychomycosis in the halluces after clinical analysis. Among them, 35/64 (54.7%) individuals presented a positive direct mycological examination and underwent fungal culture to identify the etiological agent. In this group of patients, 24/35 (68.6%) individuals who presented clinical forms whose treatment involved the need for nail debridement were selected. Only 15/24 (62.5%) individuals completed the study. Among the study participants, 5/15 (33.3%) still presented positive fungal culture in the presence of a negative direct mycological examination and 1/15 (6.7%) presented a positive direct mycological examination, but with a negative culture. Among those with a positive fungal culture, 3/15 (20.0%) participants presented microorganisms different from those isolated in the initial exams. Regarding cure, 5/15 (33.3%) participants showed a clinical response, 4/15 (26.7%) clinical cure, and 3/15 (20.0%) complete cure. No patient presented an allergic reaction or local irritation caused by the material used in the treatment. There were accidental superficial ulcerations caused by the electric sandpaper; however, no wound developed secondary infection. No participant reported discomfort due to the nail prosthesis use, 3/15 (20.0%) reported a feeling of discomfort caused by the vibration of the electric file and 12/15 (80.0%) reported the perception that their nails had a better appearance during treatment with nail prosthesis made with acrylic reconstruction gel and 2% terbinafine.
Conclusion: The application of 2% terbinafine in acrylic reconstruction gel for the manufacture of nail prostheses applied after debridement of moderate and severe forms of onychomycosis showed low efficacy as an isolated treatment in patients on dialysis due to chronic kidney disease. On the other hand, most patients had a good perception of the appearance of their nails during treatment, even when it did not result in apparent clinical improvement or complete cure.
Keywords: antifungal; clinical trial; kidney dialysis; microbiology; nail plate debridement; onychomycosis.
Copyright © 2024 Bersano, Cordeiro, Sciani, Tescarollo and Marson.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Prevalence and risk predictors of onychomycosis in patients on hemodialysis: an observation, prospective, and unicenter study in Brazil.Front Med (Lausanne). 2023 Nov 23;10:1268324. doi: 10.3389/fmed.2023.1268324. eCollection 2023. Front Med (Lausanne). 2023. PMID: 38076229 Free PMC article.
-
A multicentre, randomised, parallel-group, double-blind, vehicle-controlled and open-label, active-controlled study (versus amorolfine 5%), to evaluate the efficacy and safety of terbinafine 10% nail lacquer in the treatment of onychomycosis.Mycoses. 2022 Apr;65(4):392-401. doi: 10.1111/myc.13392. Epub 2021 Dec 6. Mycoses. 2022. PMID: 34752667 Clinical Trial.
-
Onychomycosis due to Neoscytalidium treated with oral terbinafine, ciclopirox nail lacquer and nail abrasion: a pilot study of 25 patients.Mycopathologia. 2013 Feb;175(1-2):75-82. doi: 10.1007/s11046-012-9580-5. Epub 2012 Sep 14. Mycopathologia. 2013. PMID: 22976905
-
Topical and device-based treatments for fungal infections of the toenails.Cochrane Database Syst Rev. 2020 Jan 16;1(1):CD012093. doi: 10.1002/14651858.CD012093.pub2. Cochrane Database Syst Rev. 2020. PMID: 31978269 Free PMC article.
-
Terbinafine in the treatment of onychomycosis: a review of its efficacy in high-risk populations and in patients with nondermatophyte infections.Br J Dermatol. 2004 Mar;150(3):414-20. doi: 10.1046/j.1365-2133.2003.05726.x. Br J Dermatol. 2004. PMID: 15030322 Review.
References
-
- Bodman MA, Syed HA, Krishnamurthy K. Onychomycosis. Treasure Island, FL: StatPearls Publishing; (2024). - PubMed
LinkOut - more resources
Full Text Sources