

Lexical markers of disordered speech in primary progressive aphasia and 'Parkinson-plus' disorders
- PMID: 39659971
- PMCID: PMC11630745
- DOI: 10.1093/braincomms/fcae433
Lexical markers of disordered speech in primary progressive aphasia and 'Parkinson-plus' disorders
Abstract
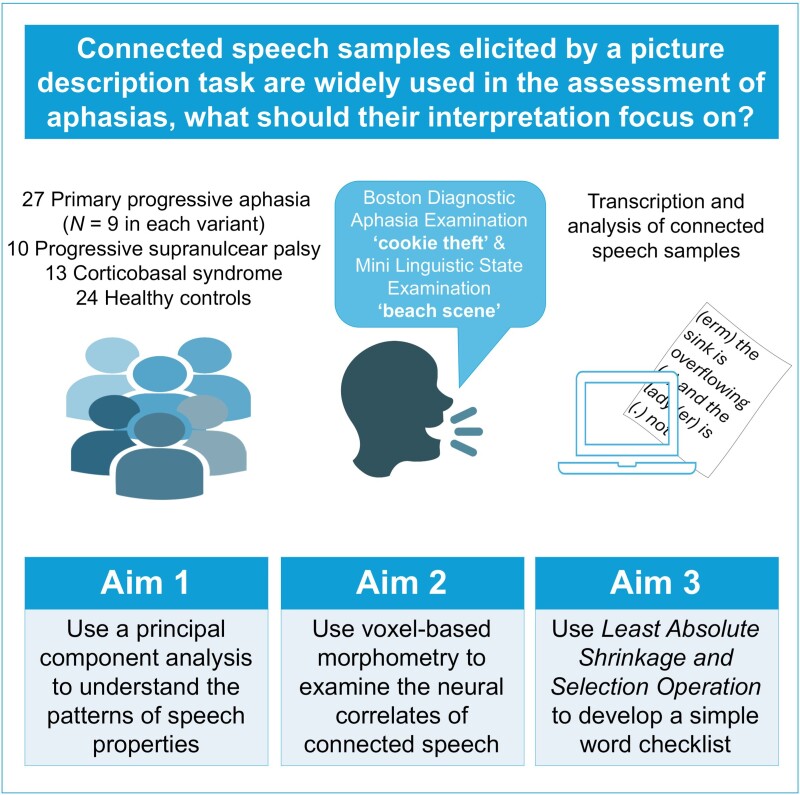
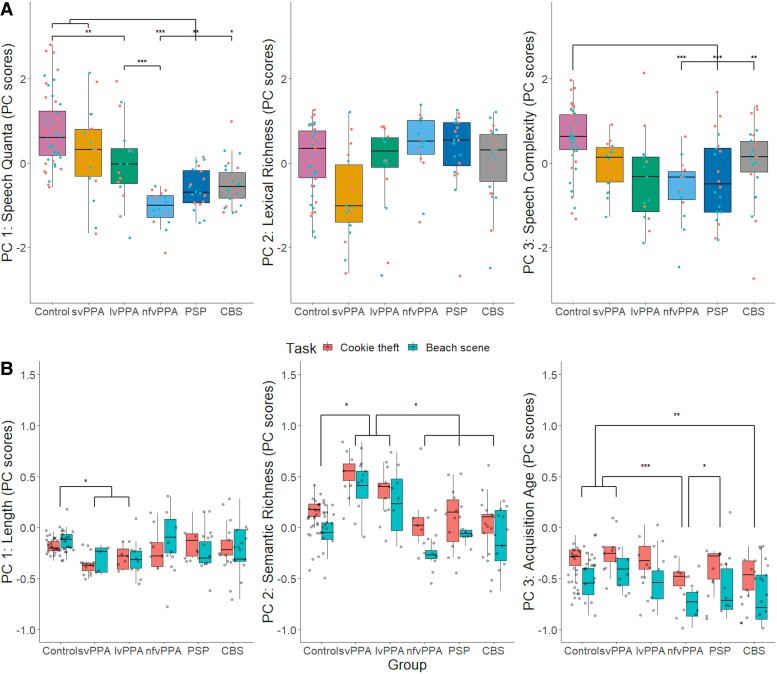
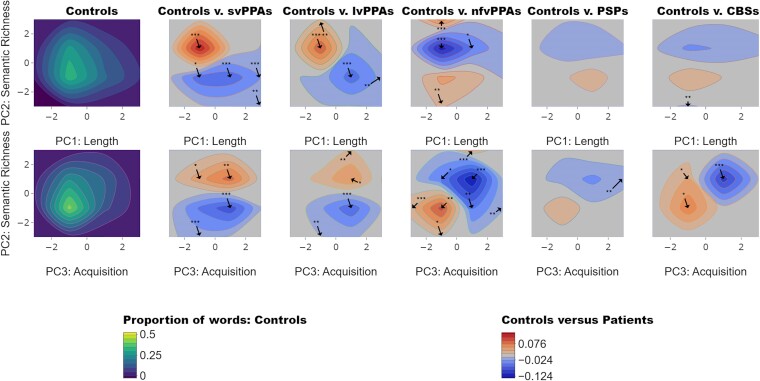
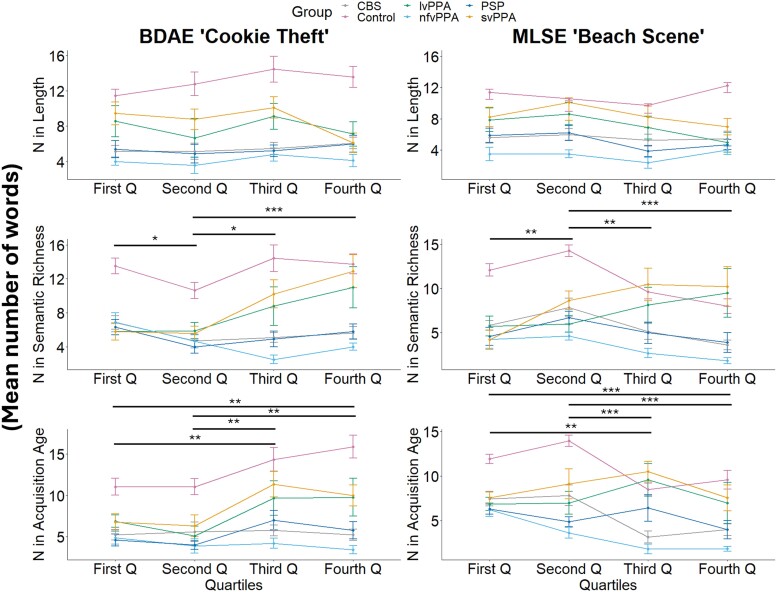
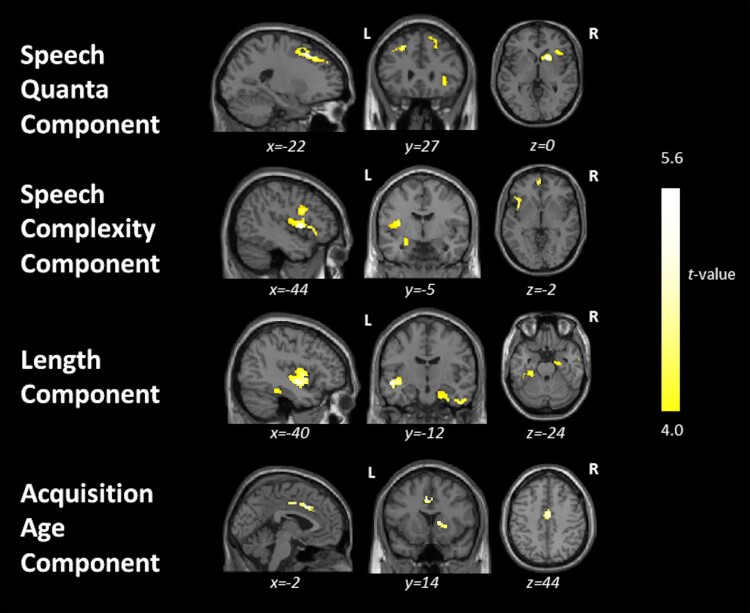
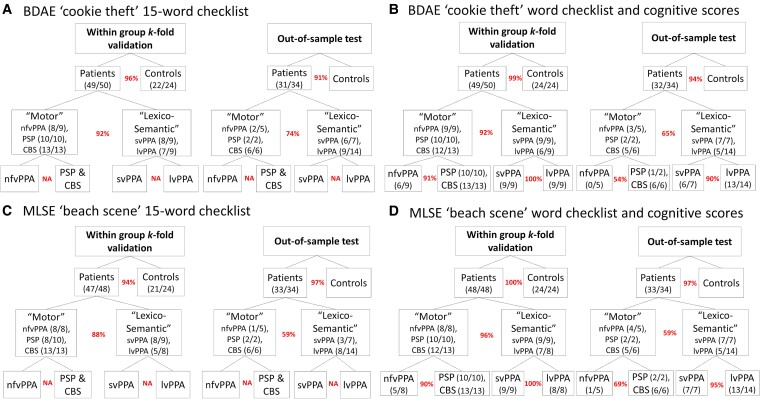
Connected speech samples elicited by a picture description task are widely used in the assessment of aphasias, but it is not clear what their interpretation should focus on. Although such samples are easy to collect, analyses of them tend to be time-consuming, inconsistently conducted and impractical for non-specialist settings. Here, we analysed connected speech samples from patients with the three variants of primary progressive aphasia (semantic, svPPA N = 9; logopenic, lvPPA N = 9; and non-fluent, nfvPPA N = 9), progressive supranuclear palsy (PSP Richardson's syndrome N = 10), corticobasal syndrome (CBS N = 13) and age-matched healthy controls (N = 24). There were three principal aims: (i) to determine the differences in quantitative language output and psycholinguistic properties of words produced by patients and controls, (ii) to identify the neural correlates of connected speech measures and (iii) to develop a simple clinical measurement tool. Using data-driven methods, we optimized a 15-word checklist for use with the Boston Diagnostic Aphasia Examination 'cookie theft' and Mini Linguistic State Examination 'beach scene' pictures and tested the predictive validity of outputs from least absolute shrinkage and selection operator (LASSO) models using an independent clinical sample from a second site. The total language output was significantly reduced in patients with nfvPPA, PSP and CBS relative to those with svPPA and controls. The speech of patients with lvPPA and svPPA contained a disproportionately greater number of words of both high frequency and high semantic diversity. Results from our exploratory voxel-based morphometry analyses across the whole group revealed correlations between grey matter volume in (i) bilateral frontal lobes with overall language output, (ii) the left frontal and superior temporal regions with speech complexity, (iii) bilateral frontotemporal regions with phonology and (iv) bilateral cingulate and subcortical regions with age of acquisition. With the 15-word checklists, the LASSO models showed excellent accuracy for within-sample k-fold classification (over 93%) and out-of-sample validation (over 90%) between patients and controls. Between the motor disorders (nfvPPA, PSP and CBS) and lexico-semantic groups (svPPA and lvPPA), the LASSO models showed excellent accuracy for within-sample k-fold classification (88-92%) and moderately good (59-74%) differentiation for out-of-sample validation. In conclusion, we propose that a simple 15-word checklist provides a suitable screening test to identify people with progressive aphasia, while further specialist assessment is needed to differentiate accurately some groups (e.g. svPPA versus lvPPA and PSP versus nfvPPA).
Keywords: Parkinson-plus disorders; connected speech; lexico-semantic word properties; picture description word checklist; primary progressive aphasia.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
The authors report no competing interests.
Figures
References
-
- Bird H, Lambon Ralph MA, Patterson K, Hodges JR. The rise and fall of frequency and imageability: Noun and verb production in semantic dementia. Brain Lang. 2000;73(1):17–49. - PubMed
-
- Hoffman P, Meteyard L, Patterson K. Broadly speaking: Vocabulary in semantic dementia shifts towards general, semantically diverse words. Cortex. 2014;55:30–42. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous