

Prenatal multidisciplinary counseling for fetal congenital anomalies: A narrative review
- PMID: 39660910
- PMCID: PMC12011073
- DOI: 10.1002/ijgo.16068
Prenatal multidisciplinary counseling for fetal congenital anomalies: A narrative review
Abstract
Introduction: Prenatal multidisciplinary counseling for fetuses with congenital anomalies involves a collaborative approach, integrating expertise from various medical fields.
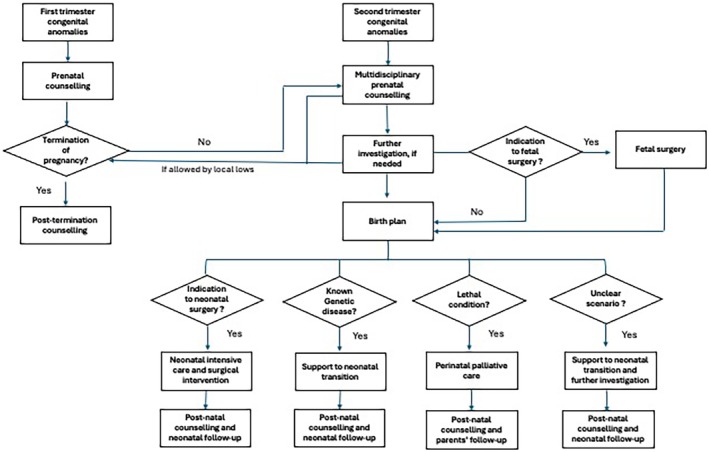
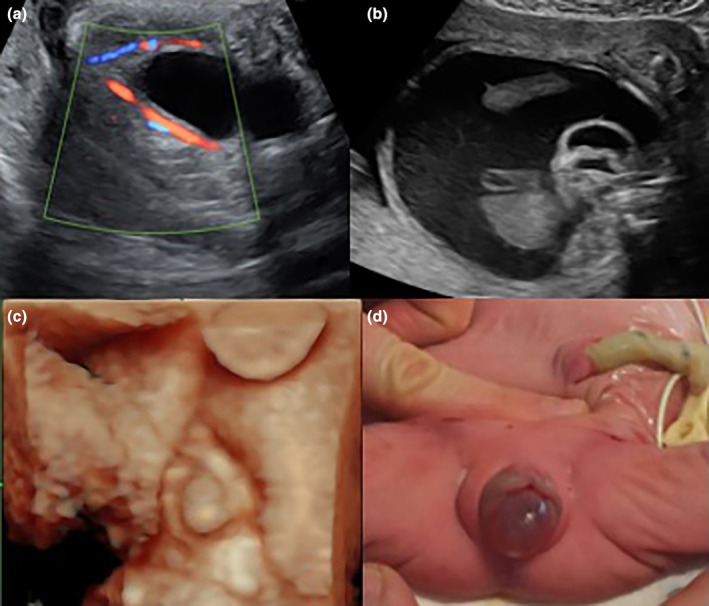
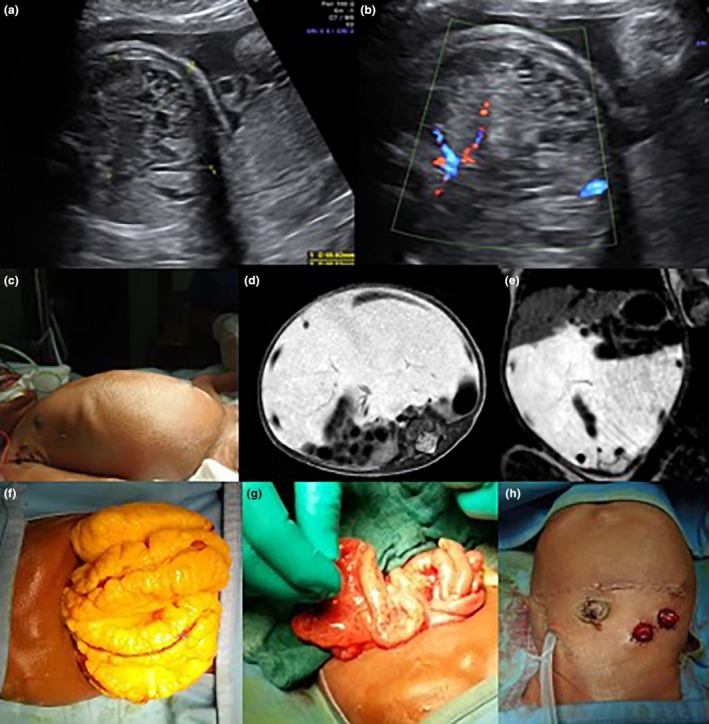
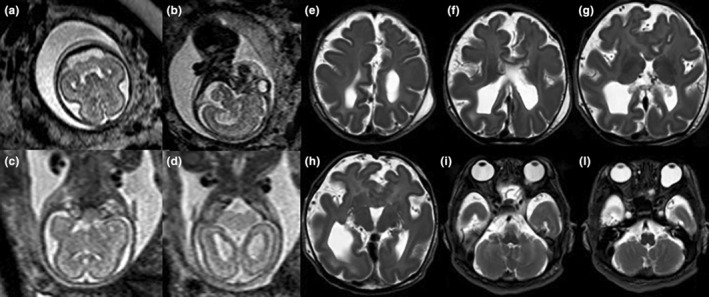
Aims and approach: This comprehensive strategy aims to provide expectant parents with accurate information about the diagnosis, potential outcomes, and available interventions. Genetic counselors, obstetricians, neonatologists, and other specialists work together to address medical, psychological, and ethical aspects. The prenatal multidisciplinary counseling approach emphasizes open communication, fostering a supportive environment for the couple to express their concerns and ask questions. In the case of prenatally detected fetal congenital anomalies, several different scenarios can be delineated: (1) detection of surgically correctable congenital anomalies, (2) identification of genetic disease or fetal anomalies likely to result in disabilities, (3) discovery of severe and lethal congenital anomalies, and (4) encountering fetal anomalies that are not well-defined, leading to an unclear scenario. The process of counseling includes discussing the possibility of pregnancy termination, treatment options, potential challenges, and emotional support, enabling expectant parents to make informed decisions aligned with their values and preferences. Additionally, the counseling process extends beyond the initial diagnosis, providing ongoing support as the pregnancy progresses and helping families to prepare for the difficulties they may face after the birth of the child with congenital anomalies. This collaborative effort not only focuses on the medical aspects but also considers the emotional and ethical dimensions of decision-making.
Conclusion: The multidisciplinary approach enhances the quality of care and empower parents, facilitating a more informed and compassionate journey throughout the prenatal period.
Keywords: congenital anomalies; prenatal diagnosis; prenatal multidisciplinary counseling.
© 2024 The Author(s). International Journal of Gynecology & Obstetrics published by John Wiley & Sons Ltd on behalf of International Federation of Gynecology and Obstetrics.
Conflict of interest statement
The authors have no conflicts of interest.
Figures
References
-
- World Health Organization . Congenital disorders. Accessed March 2024. https://www.who.int/news‐room/fact‐sheets/detail/birth‐defects
-
- Euracat technical report. 2021. https://eu‐rd‐platform.jrc.ec.europa.eu/system/files/public/EUROCAT‐Stat...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
